AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2692-9406/085
Professor, retired, USA.
*Corresponding Author: Igor Klepikov, Professor, retired, USA.
Citation: I Klepikov. (2021). Why do Patients with Acute Pneumonia Receive Intravenous Infusions?. Biomedical Research and Clinical Reviews. 5(1); DOI: 10.31579/2692-9406/085
Copyright: ©2021 Igor Klepikov. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 September 2021 | Accepted: 13 October 2021 | Published: 21 October 2021
Keywords: pneumonia; infusions; diagnosis; abdominal cavity; dogmas; synchronicity; acute disease
Currently, almost all urgently hospitalized patients immediately get access to the venous bed and begin to receive an infusion of solutions. This priority of this procedure is due not only to the need to have the most effective way of administering medications, but also to compensate for the loss of fluid, which in acute diseases has many reasons for this. Further recommendations for the correction of water-electrolyte and volume losses and the choice of the infusion rate are determined by the general criteria for their diagnosis in accordance with the parameters of the large circle of blood circulation. Considering AP, first of all, as a result of infection and not focusing on the localization of the process, modern medicine does not make exceptions in this therapeutic direction for patients with inflammation of the lung tissue.
Currently, almost all urgently hospitalized patients immediately get access to the venous bed and begin to receive an infusion of solutions. This priority of this procedure is due not only to the need to have the most effective way of administering medications, but also to compensate for the loss of fluid, which in acute diseases has many reasons for this. Further recommendations for the correction of water-electrolyte and volume losses and the choice of the infusion rate are determined by the general criteria for their diagnosis in accordance with the parameters of the large circle of blood circulation. Considering AP, first of all, as a result of infection and not focusing on the localization of the process, modern medicine does not make exceptions in this therapeutic direction for patients with inflammation of the lung tissue.
For many years, fever and tachypnea were considered the main causes of fluid deficiency in patients with AP [1]. But the role of these factors in the occurrence of inconspicuous losses is hardly worthy of comparison with the consequences of homeostasis disorders accompanying such diseases as, for example, enterocolitis or peritonitis, when the body really loses large volumes of fluid. Such losses are very noticeable and can be estimated both quantitatively and qualitatively.
Try to compare the volume and quality of losses through the gastrointestinal tract that occur as a result of repeated vomiting and diarrhea, as well as intense exudate into the intestinal lumen and into the abdominal cavity, with the evaporation of fluid during breathing and an increase in body temperature. Even if we imagine that all patients with AP during hospitalization in the hospital have a respiratory rate twice higher than normal, and the body temperature is stable at 39 degrees Celsius, the approximate loss of fluid from the body as a result of increased evaporation will not be able to approach the volume and quality of the above emissions. Nevertheless, all patients with a severe and aggressive course of the disease, regardless of the diagnosis, are recommended to inject fluid with boluses [2-5].
The differences between obvious and hidden fluid losses in patients with inflammatory processes should inevitably raise doubts that the main cause of circulatory disorders in AP is dehydration as a result of increased sweating. As is known, such hemodynamic disorders can occur at the very beginning of inflammation of the lung tissue, sometimes literally within a few hours. The unlikely role of evaporation mechanisms in the development of severe circulatory disorders in AP gave reason to interpret such aggressive forms of the disease as sepsis and septic shock [2, 4, 5].
In the literature, information about the frequency of detection of bacteria in the blood of patients with AP does not receive attention. It can be found only in isolated reports, in which the release of the pathogen from the blood of patients with this disease is only from 2-9% to 12%, including not only cases of sepsis and septic shock, but also bacteremia [6-8]. Analyzing septic complications of various diseases, some authors draw attention to the fact that bacteriological blood testing in patients with AP usually does not give results [9,10]. Even in patients with AP and septic shock, the frequency of positive blood cultures is only from 13.2% to 18%, while the comparative mortality rates from this complication with positive and negative tests do not have significant differences [11, 12].
Declaring the penetration of the pathogen into the bloodstream as the cause of severe AP does not mean that the diagnosis of septic complications corresponds to reality. However, the concept of the leading role of the pathogen in the clinical manifestations of the process requires analysis and interpretation, and such explanations are beginning to be associated with the effect of preliminary antibacterial therapy [9, 13, 14]. The paradoxical nature of this conclusion is obvious, since it turns out that, on the one hand, antibiotics effectively destroy bacteria, but, on the other hand, they are not able to prevent the development of septic complications. This strange and illogical explanation is just an attempt to bring incomprehensible facts into line with familiar dogmas.
And yet, despite the lack of objective arguments in favor of the alleged causes of hemodynamic disorders in patients with AP, such factors undoubtedly exist and manifest themselves quite quickly and hard. The use of various methods for assessing the severity of the condition of these patients shows a characteristic feature of clinical manifestations with a tendency to develop hypotension. This feature is noted with the help of widely used diagnostic methods, which include a set of different tests: APACHE II (Acute physiology and chronic health assessment II), CURB-65 (confusion, urea, respiratory rate, blood pressure, age ⩾ 65 years), PSI, the method of determining which is not much different from the first method [15-18].
A common feature of these methods, which are popular in intensive care units, for determining the severity of the condition and the prognosis of patients is that they do not reflect differences in diagnoses and localization of the main process. In addition, one of the most important tests in all severe patients is the indicator of peripheral blood pressure. This generalization of various diseases and the interpretation of disorders in accordance with the same pathogenesis scheme is the main drawback when evaluating patients with AP.
In order to understand the reason for the distorted assessment of the condition of patients with different localization of the primary focus of inflammation and to find out the origins of the signs that force intravenous infusions in AP, it is necessary to recall some fundamental canons of medicine and well-known facts.
Firstly, inflammation of the lung tissue remains the only disease among such processes that occurs in the small circle of blood circulation.
Secondly, the synchronicity of the work of the two halves of the cardiovascular system is ensured by the entry of equal volumes of blood into them and significantly lower pressure in the pulmonary vessels.
Thirdly, the violation of parity between the small and large circles of blood circulation is incompatible with life, and functional deviations that constantly occur both in the process of vital activity of the body and in the case of diseases are leveled by the autonomous regulatory system.
Fourth, the inflammatory transformation of tissues is based on a sequential step-by-step reaction of blood vessels in the affected area with a violation of blood flow and a sharp increase in the permeability of the vascular wall.
Finally, an acute inflammatory process is inevitably accompanied by five classic signs described many centuries ago by Celsus and Galen and received indisputable confirmation on the basis of subsequent medical experience: heat, pain, redness, swelling, and loss of function. Therefore, these factors will act independently of our attitude to them, and the violation of function will determine the features of the clinic of the disease, depending on the affected organ.
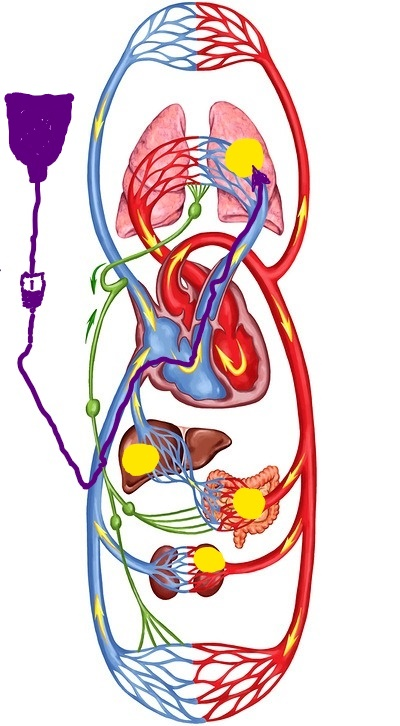
If we now take into account the presented information, the functional consequences of inflammation in the small circle of blood circulation begin to radically differ from similar processes of peripheral localization. The following diagram can give a general idea of the significance of the localization of the focus of inflammation for the blood circulation of the body (see Figure 1, Comment 1). This image is a clear proof of the fact that a sudden lesion of the lung tissue creates a physical barrier to the general blood flow, while other localizations are accompanied by a violation of blood circulation in the regional segments of the vascular network.
However, the influence of the focus of inflammation in the lung on the blood flow in the small circle of blood circulation is much more complex and broader than just a physical obstacle, depending on the volume of tissue damage. The regulation of the life balance between the two circulatory circles works independently of our desires with the slightest shifts and obstacles. For almost a century, it has been known about the presence of baroreceptors in the pulmonary vessels, the irritation of which is accompanied by their spasm and a decrease in pressure in the peripheral vessels of the large circle [19]. This reflex mechanism, known in the medical literature as the discharge reflex, is our salvation in the event of unforeseen circumstances that have arisen in the vascular pool of the lungs.
This adaptive mechanism, despite its protective nature, in the case of rapid development of pathological processes can lead to situations that themselves require immediate elimination. But now the direction of medical care is determined by the interpretation of the reasons that in this case need to be eliminated, and the result of these efforts will depend on the influence of a particular technique on the pathogenetic mechanisms of the disease.
Since hypotension in patients with AP is currently considered as a manifestation of sepsis and septic shock (see above), intravenous bolus infusions are recommended in such situations by analogy with extrapulmonary causes of septic complications [2-5]. At the same time, up to 40-50% of the total mass of septic complications are patients with AP, in which a different mechanism of circulatory disorders is the leading one [4].
The mechanism of hypotension in the large circle of blood circulation in AР as a result of damage to the pulmonary vessels was presented above, and this sign of the disease is especially manifested in the aggressive development of the process. In this situation, it is not difficult to imagine the role played by infusions that increase venous return and additional blood flow to the focus of inflammation (Fig. 2, comment 2). However, the effect of infusion therapy on the dynamics of AP is also a much more complex process than its visual version shown in the figure.
The need to clarify the role of infusion therapy in the dynamics of the development of lung inflammation arose in our work many years ago, when the most aggressive bacterial forms of AP began to be purposefully hospitalized in the our department during the initial period of the disease. The concentration of a large number of such patients was accompanied by the rapid development of pleural complications and high mortality in them. A typical example of such a development of events is our following observation.
A 2-year-old girl was taken to the clinic with abdominal pain and shortness of breath 12 hours after their appearance. According to her medical history, the child was healthy, but in the last few days she had a mild respiratory syndrome with a runny nose and a cough without fever. Upon admission to the clinic, the patient was diagnosed with AP (Fig. 2). Intensive treatment was immediately started, including intravenous administration of two antibiotics and intravenous fluids up to 30 ml / kg / hour for 2 hours, followed by a decrease in the infusion rate to 10 ml/ kg/ hour. Despite the treatment, the child's condition did not improve, and a control radiograph was diagnosed with pyopneumothorax 36 hours after hospitalization (Fig. 3). The pus obtained from the pleural cavity during drainage was subjected to bacteriological and microscopic examination, but no microflora was found in it.


There is an intense uniform darkening of almost the entire right hemithorax with a displacement of the mediastinum to the left, as well as a cavity with a fluid level in the upper pulmonary field.
The presented observation cannot be an absolute proof of the negative effect of infusion therapy on the dynamics of the inflammatory process in the lung. The results of the observed transformation in the area of inflammation only allow us to assume such a dependence and draw appropriate conclusions on an empirical basis. Therefore, in order to find additional arguments in favor of such an assumption, which cannot be obtained in clinical conditions, animal experiments were conducted.
The volume of the description of experimental studies does not allow us to present them in the framework of a journal article. However, if it is necessary to obtain this information, it can be found in available sources [20, 21]. Only the section of the study that is directly relevant to the issue under discussion is given here.
First of all, a model of the bronchogenic form of AP was created. At the same time, in order to reduce the charismatic etiology of the disease and to assess the significance of other factors, cultures of microbes that are usually not considered as pathogens of AP were used. The choice was made in favor of Escherichia coli and Staphylococcus epidermidis. When a statistically reliable stable production of the AP model was obtained, in the final series of experiments, intravenous infusions of solutions were administered to rabbits during the occurrence of inflammation in the lungs. The volume of infusions was 30 ml/kg/hour and was performed once a day for 3 days. In addition, in 6 cases, the addition of a methylene blue dye to the infusion solution was used. This technique was borrowed from the experiments of V. Mеnkin, who discovered the permeability factor [22].
The results obtained after euthanasia of animals on the fourth day of the experiment showed the following. Reproduction of the AP model without subsequent intravenous infusions was accompanied by the development of local inflammation of the lung tissue with a slight pleural reaction in some cases. Intravenous infusions in all cases were accompanied by the development of parapneumonic pleurisy. In two cases, pyopneumothorax was detected, the cause of which was small foci of destruction in the lung tissue. After infusions with the addition of dye, weakly colored lung tissues were found along the periphery of the inflammatory focus (Fig.4).
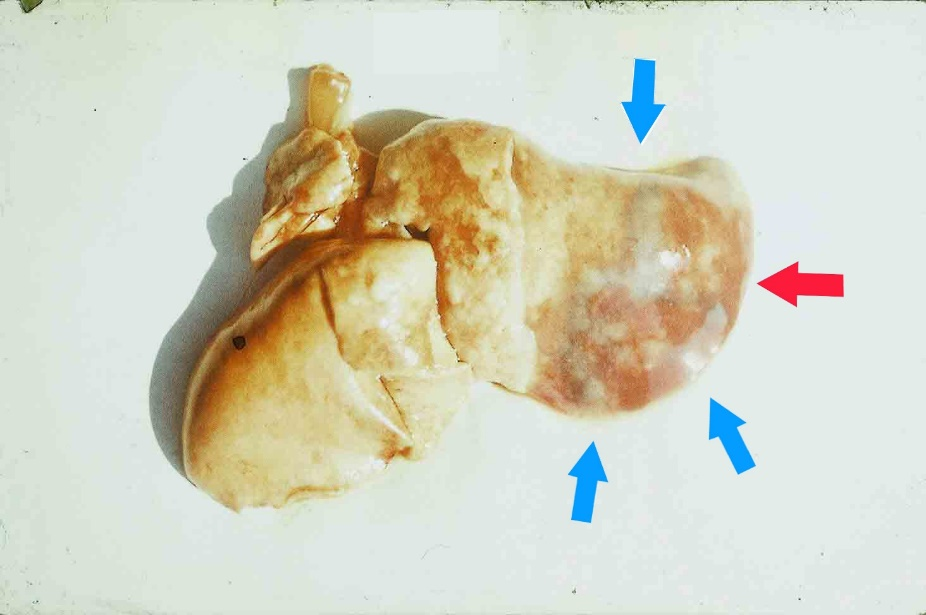
Thus, the results of the experiments allowed us to obtain additional and undoubted confirmation of the negative role of intravenous infusions in AP. The use of the dye demonstrated a visual effect of the spread of inflammatory infiltration in the lung tissue, which is a consequence of an increase in blood flow to the area with increased vascular permeability. In addition, it should be emphasized that, despite the strict repetition of the experimental conditions in each specific case, the final results were distinguished by individual diversity.
The totality of the facts presented above gave grounds to exclude any intravenous infusions in patients with AP, especially in the initial period of the disease. As an alternative to first aid for such patients, instead of infusion therapy, methods were used to relieve reflex spasm of the vessels of the small circle and at the same time reduce venous return (cupping therapy, body cooling, vagosympathetic blockade). The results of such a transformation of medical care in aggressive forms of AP exceeded our expectations [20, 21].
Unfortunately, the results of this work for a number of reasons were not presented in a timely manner in the most widespread English-language scientific literature. Today, the previous stereotypes of treating this category of patients with intravenous infusions continue to dominate in wide world practice, and the final materials indicate a continuing increase in pleural empyema in patients with AP, even in regions with developed health systems [23,24].
The additional information presented above gives an idea of one of the pathogenetic mechanisms of stimulating the inflammatory process in the lungs. Such an analysis allows us to understand why the frequency of parapneumonic effusion in community-acquired pneumonia reaches 20-50% of cases, and the empyema of the pleura can be sterile in microbiological studies [25].
The development of the SARS-CoV-2 pandemic has not changed the strategy for solving the problem of lung tissue inflammation. The causative agent of the process and its suppression continue to be the main goal of current research and therapeutic efforts. The mechanisms of the disease development are studied mainly at the cellular and molecular level. The dependence of AP manifestations on known biological rules, compensatory reactions of the body, their manifestation and the level of permissible deviations do not receive due attention in discussions and search works. After all, like A.H. Attaway and co-authors rightly point out [26], modern respiratory care revolves around auxiliary measures.
Meanwhile, the appearance of new facts only confirms the materials already passed over the past decades, in which the change in the pathogens of AP did not affect its leading characteristics. The pathogenetic mechanisms of viral pneumonia have the same basis as the bacterial forms. For example, the use of tomography in patients with COVID-19 pneumonia to determine the volume of blood in the lungs allowed us to establish a decrease in this indicator in small vessels with a diameter of no more than 2 mm [27]. The authors suggest that this fact is caused by spasm and thrombosis of small vessels as a result of their viral damage. Generalized thrombosis of this localization can hardly be compatible with life, but the spasm of the pulmonary vessels fully corresponds to the already known and mentioned above discharge reflex.
Thus, modern therapeutic efforts aimed at correcting systemic circulatory disorders are the result of an incorrect interpretation of their causes and mechanisms. The long-term fascination with the etiology of AP and the etiotropic principles of treatment has left a deep didactic trace with the oblivion of many biological laws. Bringing the concept of the disease in line with the basics of medical science should be the first stage of further revision of the complex of therapeutic measures.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation. “The peer review process was efficient and constructive, and the editorial office provided excellent communication and support throughout. The journal ensures scientific rigor and high editorial standards, while also offering a smooth and timely publication process. We sincerely appreciate the work of the editorial team in facilitating the dissemination of innovative approaches such as the Bonori Method.” Best regards, Dr. Matteo Bonori.
