
Research Article | DOI: https://doi.org/10.31579/2637-8892/229
1 Community Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt
2 Nursing Specialist Beni-Suef University, Egypt
3 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt
*Corresponding Author: Elzeblawy Hassan, Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Mohamed Saleh ASE., Mona M. Mohamed., Amal A Mohamed., Hanan Elzeblawy Hassan. (2023), Viral Hepatitis B&C In Elderly Hemodialysis Unit: Nurses' Related Knowledge, Psychology and Mental Health Care, 7(6): DOI:10.31579/2637-8892/229
Copyright: © 2023, Hanan Elzeblawy Hassan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 August 2023 | Accepted: 11 September 2023 | Published: 18 September 2023
Keywords: viral hepatitis b&c; elderly; hemodialysis nurses' knowledge
Background: Worldwide, 480-520 million people is living with viral hepatitis. Globally, an estimated 78% of primary liver cancer and 57% of liver cirrhosis cases are caused by viral hepatitis, and 1 million deaths from viral hepatitis occur each year. Chronic hepatitis B and C are among the leading causes of infectious-disease death worldwide. Egypt’s MOHP is committed to ensuring that new cases of viral hepatitis are prevented and that persons who are already infected are tested; informed about their infection; and provided with counseling, care, and treatment. Aim: The aim of this study was to assess nurses' knowledge regarding preventive measures for viral hepatitis B & C in hemodialysis dialysis unit.
Design: A descriptive exploratory design was utilized in the current study. Setting: The study was carried out in two hemodialysis units at Beni-Suef University Hospital and Elwasta General Hospital in Beni-Suef Governorate. Subjects: A convenient sample of 76 hemodialysis nurses, of whom 22 were men and 54 women, and who provided direct patient care, consented to take part in the study. Results: The mean of age is 23.45±2.71 years, 52.6% of the dialysis nurses have technical institute, and 48.7% of the dialysis nurses have 2-5 years of experience in nursing field. For dialysis nurses' knowledge about elderly, viral hepatitis B & C, infection control for elderly patients in dialysis unit; 50.0% & 51.3% of them have fair level of knowledge about elderly and viral hepatitis, respectively. Moreover, 52.6% & 55.3% have fair level of knowledge about general knowledge about general and specific preventive measures of infection control in dialysis unit, respectively. Furthermore, 52.6% of the dialysis nurses have fair level of knowledge about infection control standards for dialysis patients. Also 85.5% of the dialysis nurses have good level of knowledge about practices toward viral hepatitis B&C in dialysis unit.
Conclusion: There is statistically significant relation between dialysis nurses' knowledge and their education level, training program for new dialysis nurses, training program for improving nursing skills and participate in educational lectures before, age, years of experience in nursing field, years of experience in dialysis unit, the opportunity to view the courses and medical journals and participate in scientific conferences for dialysis and kidney disease during the last 5 years.
Recommendations: Conducting standards educational program that emphasize on improving knowledge level regarding prevention of viral hepatitis transmission in HDUs in order to raise awareness and correct misconceptions.
Although high-income countries have the highest costs for dialysis and kidney transplantation, fewer than one (29%) in three high-income countries consider chronic kidney disease a priority compared with almost two (59%) in three low-in-come countries [1]. Acute kidney injury (AKI) is a syndrome characterized by a rapid (hours to days) deterioration of kidney function. It is often diagnosed in the context of other acute illnesses and is particularly common in critically ill patients. The clinical cones less obvious effects, including reduced immunity and dysfunction of non-renal organs (organ crosstalk) chronic kidney disease (CKD) is a global health burden with a high economic cost to health systems and is an independent risk factor for cardiovascular disease (CVD). All stages of CKD are associated with increased risks of cardiovascular morbidity, premature mortality, and/or decreased quality of life [2]. Worldwide, about 1 in every 12 persons (480-520 million people) is living with viral hepatitis. Globally, an estimated 78% of primary liver cancer and 57% of liver cirrhosis cases are caused by viral hepatitis, and 1 million deaths from viral hepatitis occur each year. Chronic hepatitis B and C are among the leading causes of infectious-disease death worldwide. The proportion of persons living with viral hepatitis is greatest in Asia, Sub-Saharan Africa, and Egypt; however, prevalence of HCV infection is high among subpopulations (e.g., people who inject drugs [PWIDs] and persons living in correctional settings) in almost all parts of the world [3]. Egypt’s MOHP is committed to ensuring that new cases of viral hepatitis are prevented and that persons who are already infected are tested; informed about their infection; and provided with counseling, care, and treatment. The Plan of Acton will help the MOHP improve its current efforts to prevent viral hepatitis and related disease by 1) identifying steps that can be taken to reach specific goals; 2) leveraging opportunities to improve coordination of viral hepatitis activates across MOHP sectors; 3) setting priorities for MOHP to develop public-health and primary care infrastructure needed for viral hepatitis prevention across all sectors; and 4) providing a framework for MOHP to engage other governmental agencies and nongovernmental organizations (NGOs) in viral hepatitis prevention and care [4].
The aim of this study was to assess nurses' knowledge regarding preventive measures for viral hepatitis B & C in hemodialysis dialysis unit
2.1. Research Questions
What about hemodialysis nursing staffs' knowledge regarding preventive measures for viral hepatitis B & C in hemodialysis dialysis unit?
3.1 Subjects & Setting:
In the Beni-Suef governorate, the study was carried out in two hemodialysis units at Elwasta General Hospital and Beni-Suef University Hospital. Ground level of Beni-Suef University Hospital housed the first unit. The nurse-to-patient ratio is between 1:3 and 1:4. The second unit was in the general hospital in Elwasta with a nurse-to-patient ratio of 1:3 or 1:4. The goal of the investigation was achieved through a descriptive exploratory study. All 76 hemodialysis nurses, of whom 22 were men and 54 women, and who provided direct patient care, consented to take part in the study. An easy sample was chosen.
3.2. Tools of Data Collection:
After reading national and international related literature reviews that related to the study issue, the researcher prepared an interview questionnaire that was created to gather information for the study.
Part I: Questionnaire about background traits: This section was created by the researcher to gather information about the background information of nurses, including their experience in dialysis units, participation in training programmes to advance their nursing skills, access to courses and medical journals, and participation in conferences for dialysis and kidney disease over the previous five years.
Part II: Nurses' knowledge: regarding elderly patients, viral hepatitis B and C in dialysis units that introduced to Nurses' understanding about viral hepatitis transmission.
The survey had 54 questions and a total of 108 grades; a complete accurate response received a two-point score, an incomplete correct response received a one-point rating, and a wrong answer or don't know received a zero-point rating. These results were added up to create a % score. It was divided into three groups: Good knowledge if score ≥ 75%, Fair knowledge if score 50-< 75%, and Poor knowledge if score from <50>
3.2.1. Validity and reliability of tool
This phase began with the preliminary phase, which focused on a review of recent and older, national and worldwide related material regarding the study's subjects using textbooks, articles, journals, and websites. With the use of this review, the investigator was able to evaluate and create data collection tools. The investigator then used his or her experience to evaluate the tools' accuracy, relevance, and correctness. The Self-administered Questionnaire was given to the nurses who volunteered to take part in the study in order to gather information about their understanding of the prevention of viral hepatitis transmission in HD units. Each nurse had to wait for a few minutes while the researcher clarified any complicated questions throughout all working shifts. A pilot study was conducted on 10% of the entire study sample (8 nurses) in order to check the tools' applicability, effectiveness, and clarity as well as the fieldwork's viability and to look for any potential challenges that the researcher might encounter. To include the pilot sample among the study subjects, modifications were made. The primary study sample was made up of the pilot sample.
The study's data collection process takes five months. The study's data collection process began at the beginning of January 2022 and was finished by the end of May 2022. The researcher visited the HD unit at Elwasta General Hospital and Beni-Suef University Hospital. Nurses work three days a week from 9 am to 12 pm; one day per hospital.
The researcher initially clarified the study's objectives with the nurses and assured them that any information gathered would be treated in confidence and would only be utilised for research purposes. The researcher interviewed nurses working in the HD unit at Elwasta General Hospital, part of Beni-Suef University Hospital.
3.4. Ethical Considerations:
The Beni-Suef University Faculty of Nursing's scientific research ethical committee gave its clearance before the study was carried out. To explain the purpose of the study and obtain their agreement, the researcher visited with the director of Elwasta General Hospital, which is affiliated with Beni-Suef University. The researcher also visited with nurses to discuss the goals of the study and get their consent to take part. They received assurances on the confidentiality and anonymity of the data obtained, which was exclusively utilised for scientific study. The nurses' freedom to leave the study at any moment was guaranteed.
A main permit was approved for ethical concerns by the hospital management as well as the research ethics committee at the faculty of nursing. Each eligible individual was told of the purpose and significance of the study at the initial interview as well. The researcher made particular to explain that participation in the study was completely voluntary and that the data were coded to ensure anonymity and confidentiality. Each participant in the study who gave their written consent was gathered.
3.5. Administrative design:
The dean of the nursing faculty at Beni-Suef University wrote an official letter to the hospital serving the university, Elwasta General Hospital, requesting their permission to perform the study. To obtain their consent and assistance with data collection, this letter included the purpose of the study as well as copies of the data collection instruments.
3.6. Statistical design:
The Statistical Package for Social Science (SPSS) version 25 computer programme and Microsoft Excel were used to conduct the statistical analysis of the data. For categorical data, frequencies and percentages were used, while for quantitative data, the arithmetic mean (X) and standard deviation (SD) were used. Data were presented using descriptive statistics. In order to compare qualitative variables, the chi square test (X2) 2, P-value, Pearson correlation test (R-test), and correlation between the study variables were all used. The following levels of findings significance were taken into consideration. Degrees of significance of results were considered as follows: P-value > 0.05 Not significant (NS), P-value ≤ 0.05 Significant (S), and - P-value ≤ 0.01 Highly Significant (HS).
Hepatitis B virus (HBV) and hepatitis C virus (HCV) infections are important causes of morbidity and mortality of hemodialysis (HD) patients. HBV and HCV prevalence in our HD patients is still high. These data emphasize the need for stricter adherence to infection control, barrier precaution and preventive behaviors with all patients. In patients on maintenance HD, the risk of hepatitis is still a serious problem despite the availability of serological tests and vaccines for hepatitis B virus infection and universal precaution standards and infection control measures. Available data suggest that HCV has become the most common cause of acute hepatitis in dialysis patients and dialysis staff members, following the implementation of infection control measures for HBV [5]. Regarding total level of knowledge related to viral hepatitis B&C for elderly patient in dialysis unit, the current study finding revealed that a large percent of the dialysis nurses have good level of total knowledge about practices and attitude to limit the spread of viral hepatitis B&C in dialysis unit. Also, about half of them have fair level of total knowledge about elderly and viral hepatitis, respectively. Moreover, more than half of them have fair level of total knowledge about general knowledge about preventive measures of infection control in dialysis unit and infection control inside dialysis unit, respectively. Furthermore, half of the dialysis nurses have fair level of total knowledge about viral hepatitis B & C for elderly patients in the dialysis units.
In the same line, a study done by bboud, & Wanner (2021) entitled “Health care workers and prevention of hepatitis B& C virus transmission” explored knowledge, attitudes and evidence-based practices in hemodialysis units in Italy [6]. All 37 HDUs of Calabria were included in the study and all nurses were invited to participate in the study. Results showed that the degree of knowledge was totally satisfactory. Another study consistent with the study findings was done by Gesualdo, et al., (2021), which assessed knowledge of viral infection among nursing staff of the Medical College of Bitola, Macedonia, southeastern Europe. Results showed that they have a sufficient knowledge about HBV& HCV to face future challenges. The investigator noticed that the last studies showed better results than that of the current study findings, and this may be due to regular attendance to theoretical and practical classes. It is worth mentioning that findings of the current study revealed that (74.5 %) received inservice training programs, while (68.29 %) received that program within the last 6 months [7]. Comply with hand hygiene requirements. Scrub the access port or hub with friction immediately prior to each use with an appropriate antiseptic Use only sterile devices to access catheters. Immediately replace dressings that are wet, soiled, or dislodged. Perform routine dressing changes using aseptic technique with clean or sterile gloves. Change gauze dressings at least every two days or semipermeable dressings at least every seven days. For patients 18 years of age or older use a chlorhexidine impregnated dressing with cleared label that specifies a clinical indication for reducing for short-term non-tunneled catheters infection unless the facility is demonstrating success at preventing infection with baseline prevention practices. Change administrations sets for continuous infusions no more frequently than every 4 days, but at least every 7 days. Promptly remove unnecessary central lines. Perform daily audits to assess whether each central line is still needed [8-9]. The finding of the present study showed that there was highly significant statistical relation between nurses' knowledge and educational level, training program for new dialysis nurses, training program for improving nursing skills and participate in educational lectures before at (P= < 0 xss=removed xss=removed> 0.05). This finding is supported by a study done by (Cekin,Y. &Ozdemir,2021) that revealed no significant difference between the hospital units in terms of the attitudes of health care workers (HCWs) toward HBV/HCV infections and their level of education. On the contrary, Joukar et al., (2020) concluded that there was a significant relation between knowledge score and age, gender, occupational history, and educational history [10].
There is statistically significant relation between dialysis nurses' knowledge and their education level, training program for new dialysis nurses, training program for improving nursing skills and participate in educational lectures before, age, years of experience in nursing field, years of experience in dialysis unit, the opportunity to view the courses and medical journals and participate in scientific conferences for dialysis and kidney disease during the last 5 years.
Conducting standards educational program that emphasize on improving knowledge level regarding prevention of viral hepatitis transmission in HDUs in order to raise awareness and correct misconceptions.
Figure (1): Presents frequency distribution of the dialysis nurses according to their socio-demographic characteristics. It shows that, (51.3%) of the dialysis nurses their age ranged between 20-<25>
Table (1) & Figure (2): present dialysis nurses' knowledge about elderly, viral hepatitis B & C, infection control for elderly patients in dialysis unit. They illustrate that 50.0% & 51.3% of them have fair level of knowledge about elderly and viral hepatitis, respectively. Moreover, 52.6% & 55.3% of them have fair level of knowledge about general knowledge about general and specific preventive measures of infection control in dialysis unit and infection control inside dialysis unit, respectively. Furthermore, 52.6% of the dialysis nurses have fair level of knowledge about infection control standards for dialysis patients. Also 85.5% of the dialysis nurses have good level of knowledge about practices toward viral hepatitis B&C in dialysis unit.
Table (2): presents relationship between socio-demographic characteristics of the dialysis nurses and their knowledge about viral hepatitis B & C for elderly patients in the dialysis units. It shows that, there is highly statistically significant relation between dialysis nurses' knowledge and their education level, training program for new dialysis nurses, training program for improving nursing skills and participate in educational lectures before at (P= < 0 xss=removed xss=removed> 0.05).
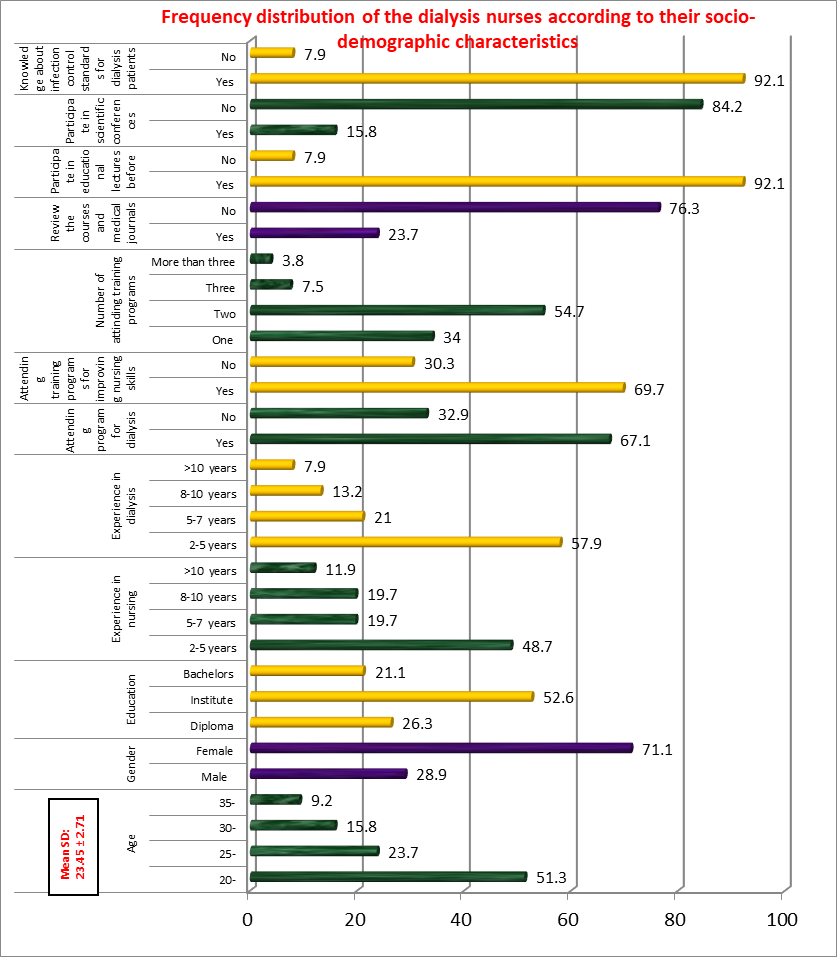
Figure (1): Frequency distribution of the dialysis nurses according to their socio-demographic characteristics (n=76)
Table (1): Frequency distribution of the dialysis nurses according to their knowledge about viral hepatitis B & C for elderly patients in the dialysis units (n=76).
| Items | Good | Fair | Poor | |||
| No. | % | No. | % | No. | % | |
| Knowledge about elderly | 24 | 31.6 | 38 | 50.0 | 14 | 18.4 |
| Knowledge about viral hepatitis | 24 | 31.6 | 39 | 51.3 | 13 | 17.1 |
| Knowledge about general precautions for infection control in dialysis unit | 28 | 36.9 | 40 | 52.6 | 8 | 10.5 |
| Knowledge about specific precautions for infection control in dialysis unit | 21 | 27.6 | 42 | 55.3 | 13 | 17.1 |
| Knowledge about practices toward viral hepatitis B&C in dialysis unit | 65 | 85.5 | 8 | 10.5 | 3 | 4.0 |
| Knowledge about infection control standards for dialysis patients | 11 | 14.5 | 40 | 52.6 | 25 | 32.9 |

Figure (2): Frequency distribution of the dialysis nurses according to their knowledge about viral hepatitis B & C for elderly patients in the dialysis units (n=76).
| Socio-demographic characteristics | Levels of total knowledge | X2
| P- Value | ||||||
| Good (n=25) | Fair (n=42) | Poor (n=9) | |||||||
| No. | % | No. | % | No. | % | ||||
Age (years) | 20- | 6 | 24.0 | 29 | 69.0 | 4 | 44.5 | 11.25 | 0.046* |
| 25- | 10 | 40.0 | 6 | 14.3 | 2 | 22.2 | |||
| 30- | 4 | 16.0 | 5 | 11.9 | 3 | 33.3 | |||
| 35 | 5 | 20.0 | 2 | 4.8 | 0 | 0.0 | |||
| Gender | Male | 7 | 28.0 | 10 | 23.8 | 5 | 55.6 | 5.341 | 0.091 |
| Female | 18 | 72.0 | 32 | 76.2 | 4 | 44.4 | |||
| Education level | Diploma | 2 | 8.0 | 11 | 26.2 | 7 | 77.8 | 18.76 | 0.000** |
| Technical | 9 | 36.0 | 29 | 69.0 | 2 | 22.2 | |||
| Bachelor | 14 | 56.0 | 2 | 4.8 | 0 | 0.0 | |||
| Years of experience in nursing field | 2- | 6 | 24.0 | 26 | 61.9 | 5 | 55.6 | 13.50 | 0.032* |
| 5- | 8 | 32.0 | 5 | 11.9 | 2 | 22.2 | |||
| 8- | 6 | 24.0 | 7 | 16.7 | 2 | 22.2 | |||
| 10- | 5 | 20.0 | 4 | 9.5 | 0 | 0.0 | |||
| Years of experience in dialysis unit | 2- | 6 | 24.0 | 33 | 78.6 | 5 | 55.6 | 14.01 | 0.025* |
| 5- | 10 | 40.0 | 4 | 9.5 | 2 | 22.2 | |||
| 8- | 5 | 20.0 | 3 | 7.1 | 2 | 22.2 | |||
| 10- | 4 | 16.0 | 2 | 4.8 | 0 | 0.0 | |||
| Training program for new dialysis nurses | Yes | 25 | 100.0 | 24 | 57.1 | 1 | 11.1 | 18.11 | 0.000** |
| No | 0 | 0.0 | 18 | 42.9 | 8 | 88.9 | |||
| Training program for improving nursing skills | Yes | 25 | 100.0 | 28 | 66.7 | 0 | 0.0 | 18.93 | 0.000** |
| No | 0 | 0.0 | 14 | 33.3 | 9 | 100 | |||
| Opportunity to view the courses and medical journals | Yes | 18 | 72.0 | 0 | 0.0 | 0 | 0.0 | 13.04 | 0.013* |
| No | 7 | 28.0 | 42 | 100 | 9 | 100 | |||
| Participate in educational lectures before | Yes | 18 | 72.0 | 0 | 0.0 | 0 | 0.0 | 16.37 | 0.000** |
| No | 7 | 28.0 | 42 | 100.0 | 9 | 100.0 | |||
| Participate in scientific conferences for dialysis and kidney disease during the last 5 years | Yes | 12 | 48.0 | 0 | 0.0 | 0 | 0.0 | 13.40 | 0.011* |
| No | 13 | 52.0 | 42 | 100 | 9 | 100 | |||
| Know the infection control standards for dialysis patients | Yes | 25 | 100.0 | 42 | 100.0 | 3 | 33.3 | 15.63 | 0.000** |
| No | 0 | 0.0 | 0 | 0.0 | 6 | 66.7 | |||
No significant at p > 0.05. *Significant at p ‹ 0.05. **highly significant at p ‹ 0.01.
Table (2): Relationship between socio-demographic characteristics of the dialysis nurses and their knowledge about viral hepatitis B & C for elderly patients in the dialysis units (n=76).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
