
Research Article | DOI: https://doi.org/10.31579/2640-1053/026
*Corresponding Author: Eduardo Harendza, Beast Oncology Services, Mexico
Citation: Eduardo Harendza, Treatment of locally advanced non-small cell lung cancer with our institutional protocol of split course concurrent chemo irradiation. J Cancer Research and Cellular Therapeutics, Doi:10.31579/2640-1053/026
Copyright: © 2018 Eduardo Harendza, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 January 2018 | Accepted: 20 February 2018 | Published: 02 April 2018
Keywords: radiation pneumonitis; pulmonary fibrosis; non-small cell lung cancer
Purpose: We sought to identify factors predictive of development of radiation pneumonitis and pulmonary fibrosis following split course concurrent chemo irradiation for locally advanced non-small cell lung cancer (LA-NSCLC).
Methods and Materials: We reviewed records of 108 patients treated with regimen of split course radiotherapy (median 60 Gy in 30 fractions) and concurrent chemotherapy for stage IIIa/IIIb NSCLC. Fisher's Exact Test and Paired Student T Test were performed to identify factors predictive of development of any pulmonary toxicity (pneumonitis or fibrosis of any grade) and severe pulmonary toxicity (grade 3 or higher pneumonitis, grade 2 or higher fibrosis).
Results: 56 patients (51.2%%) developed any toxicity; 22 patients (20.4%) developed severe toxicity. The following predictive factors were identified for any and severe pulmonary toxicity, respectively: reactive airway disease (RAD), age, RV % expected (EXP), PEF %EXP, FEV1/FVC ratio, smoking status; and RAD, FEV1 %EXP, FVC %EXP, FEV1/FVC %EXP, RV %EXP, FEF25/75 %EXP, PEF %EXP, S-GAW %, FEV1, FVC, and FEV1/FVC .
Conclusions: Our overall rates of any and severe pulmonary toxicity are acceptable. History of RAD and active smoking are protective, whereas patients with severe COPD have increased risk. A trend was seen toward improved outcomes with the use of prophylactic steroid control medication. These results should be confirmed in the context of a prospective study.
Radiation therapy (RT) remains an important component of the treatment of non-small cell lung cancer (NSCLC) [1-3]. Unfortunately, the use of RT in this context is limited by toxicity to normal tissues, particular normal lung and esophagus [4-8]. Radiation-induced pulmonary damage typically manifests as radiation pneumonitis (RP), pulmonary fibrosis (PF), or both [6,8]. A number of prior studies have evaluated clinical and dosimetric predictive factors for these toxicities, with mixed results [9-14].
At our institution, patients with locally advanced NSCLC are treated either in the definitive setting to 60Gy in 30 fractions or neoadjuvant setting to 44Gy in 22 fractions with a regimen of split course concurrent chemotherapy and RT. The specific details and clinical outcomes of this regimen have been previously published [15-16]. In this study, we sought to identify clinical features predictive of any pulmonary toxicity (versus none) and/or severe pulmonary toxicity (NCIC CTC Grade 3 or higher RP and/or Grade 2 or higher PF) versus none-mild toxicity using this regimen.
After obtaining Institutional Review Board approval for this study, we identified 108 patients treated for stage IIIa or IIIb (AJCC 7th edition) NSCLC with an institutionally developed protocol of split course concurrent chemotherapy and RT using a split course approach. RT was delivered using standard fractionation (1.8-2 Gy once daily, 5 fractions/week), 7 or 8 fractions per cycle, 21 consecutive calendar days per cycle. The total delivered dose was typically 60Gy by 2Gy fractions (65 cases), with the remaining patients receiving slightly higher or lower doses due to tumor control or toxicity concerns. These patients were selected from a larger cohort of 144 patients treated with this definitive regimen at our institution; however, 36 patients received a truncated course of treatment due to toxicity, tumor progression, or a decision to proceed with surgical resection. We excluded those patients from this analysis to improve the dosimetric homogeneity of the study population.
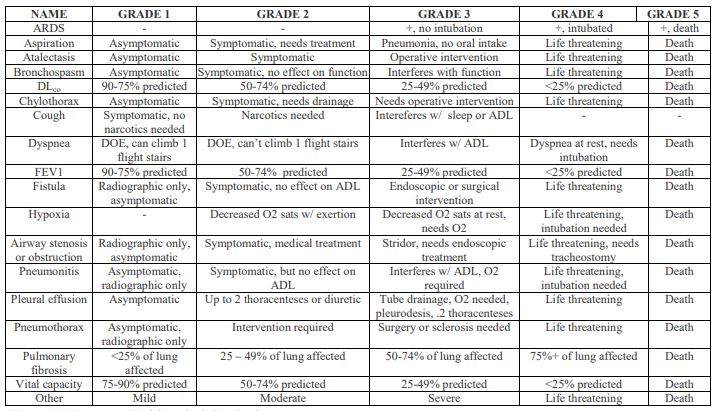
Treatment records were reviewed to obtain toxicity data from all cases. In all cases, toxicity was graded using the NCI Common Toxicity Criteria Version 3 (Figure 1 ).
We classified Grade 3 or worse RP and Grade 2 or worse PF as severe toxicity. For patients who had pulmonary function tests (PFT) performed prior to the initiation of treatment, we collected all available parameters. In cases where multiple PFTs were performed, we recorded those most immediately preceding treatment. COPD was graded using GOLD Criteria [17]. For patients administered bronchodilators during testing, an improvement in FEV1, FVC, or FEV1/FVC ratio of 12% or more or an improvement in FEF25/75 of 32% or more was classified as reversible obstructive lung disease (ROLD) [18]. Any form of documented underlying lung disease (asthma, COPD, etc.) was recorded. Patients who were taking scheduled controller medications for their underlying lung disease at the time of treatment were also identified, and the controller medication was classified as steroid-based (oral or inhaled), non-steroid based, or both (albuterol inhalers or nebulizers used as needed only were not included). Patients who initiated the use of such medications after the beginning of treatment were not included. Patients with a history of asthma or PFTs showing ROLD were classified as having reactive airway disease (RAD) [18]. We additionally noted the patients' age, the side of the primary tumor (left versus right), and the patient's smoking history. Patients were classified as never smokers, former smokers (if they quit smoking prior to the initiation of treatment), or active smokers (those who smoked during and/ or after treatment).
Dosimetric data from RT treatment plans were also reviewed for all cases. A full dosimetric analysis will be submitted in a separate manuscript. An analysis of chemotherapy-related risk factors will also be reported separately. Fisher's Exact Test was used to compare categorical variables, and Paired Student's T Test to compare continuous variables/ means, between patients who developed any pulmonary toxicity versus no pulmonary toxicity, and between patients who developed severe pulmonary toxicity versus none to mild toxicity. P values .05 or less were considered statistically significant.
56/108 patients (51.2%) developed some degree of pulmonary toxicity, while 22/108 patients (20.4%) developed severe toxicity. The following predictive factors were identified for any pulmonary toxicity versus none: history of reactive airway disease (RAD), age, high or intermediate risk dosimetry, RV % expected (EXP), PEF %EXP, FEV1/FVC ratio, and smoking status. For severe pulmonary toxicity the following factors were predictive: RAD, FEV1 %EXP, FVC %EXP, FEV1/FVC %EXP, RV %EXP, FEF25/75 %EXP, PEF %EXP, S-GAW %, FEV1, FVC, and FEV1/FVC.
A history of RAD was found to be protective against any toxicity (p .04) and severe toxicity (p .03). When a history of RAD was compared to a history of COPD, RAD was found to be borderline significant in terms of protection against any toxicity (p .08) and statistically significant for protecting against severe toxicity (p .03). A history of any COPD was not predictive of any or severe toxicity (p .27 and .90, respectively), nor was it predictive after stratification by Goldman Criteria (severe, moderate, mild) although moderate to severe disease did approach significance when compared with none to mild disease for any toxicity (p .06).
Steroid controllers did reduce the rate of any toxicity compared to no controller medication (30% versus 54%), but this difference did not reach statistical significance (p .13), likely due to the small number of patients who took steroid controller medication during their treatment. There was clearly no difference in rates of severe toxicity (19% versus 20%, p .70).
The use of non-steroid controller did not affect rates of any or severe toxicity when compared with no controller (p .44 and .90, respectively) or steroid controller (p .36 and .46, respectively). Tumor location (right versus left) did not predict for any or severe toxicity, although there was a trend toward higher rates of any toxicity for left sided tumors (p .08). These data are shown in Tables I and II.
While esophagitis and fatigue are the most commonly reported acute toxicities in the treatment of thoracic malignancies, the most common and rate-limiting subacute and late toxicity remains pulmonary [6,8-9,11,13-14]. Prior studies have identified a number of clinical and dosimetric factors which are predictive for the development of subsequent RP and PF [9-14,19-21]. The results of these studies have been mixed and sometimes contradictory, with some implicating dosimetric factors such as
various Vdose or mean lung dose (ipsilateral or bilateral) and others implicating clinical factors such as smoking status, a history of COPD, age, tumor location, and various PFT metrics [9-14,19-22]. We are unaware of any prior studies that have evaluated the relationship between a history of asthma/RAD and the risk of subsequent RP or PF. Prior studies have also shown conflicting results with regard to the prophylactic use of steroids (oral or inhaled) as a preventive measure against the development of RP or PF [13-14,23].
A recent growing body of evidence implicates the central role of TGF beta and other cytokines in the development of RP and PF [24-30]. Unfortunately, this testing is not routinely available at our institution, and thus we cannot correlate baseline or subsequent cytokine levels with the development of RP or PF in our series. It is interesting to note that in our study both a history of RAD and current smoking status (defined as active smoking during treatment with or without continued smoking after treatment) were found to be protective against the development of RP and PF, because both conditions are known to be associated with elevated basal circulating TGF beta levels [31-33]. Also, both conditions are known to favor a TH2 immunologic response to noxious stimuli, while the dominant pathway leading to upregulation of TGF beta involves a TH1 response [34-39]. While a history of RAD has not specifically been evaluated as a predictive factor for RP or PF in prior studies, the influence of cigarette smoking on the development of RP and PF has shown conflicting results in prior studies, with some showing an increase in risk, others no relationship, and still others a protective effect [12, 40-42]. These differences in outcome may reflect differences in the definition of current versus former smoking status utilized in these prior studies [40-42]. It is tempting to speculate that the upregulation of TH2 responses in the lungs of active smokers and patients with RAD may be preventing or ameliorating increases in TGF beta during treatment and thereby protecting against the development of subsequent toxicity, but this relationship cannot be proven in this study as we do not have TGF beta levels available for review.
We did not find a significant relationship between a history of COPD and the subsequent development of RP or PF for all patients, but we did find a correlation between moderate to severe disease as defined by the GOLD Criteria and the development of toxicity [18]. Prior studies have shown mixed results as regards this correlation, and these differences may be explained by differences in the definition of COPD (prior clinical diagnosis versus assessment of PFT data) and whether disease severity was specified as in this study [9,13,19,21]. We did find very strong correlations between a number of PFT metrics and the risk of developing toxicity, and these metrics including measures of spirometry (absolute and/or percent expected FVC, FEV1, FEV1/FVC ratio, PEF, and FEF 25/75), lung volumes (absolute and/or percent expected TLC, RV, and ERV), measures of resistance (GAW), and respiratory muscle force (VC MAX). Thus, it may be the actual degree of lung dysfunction rather than a definition of COPD per se which predicts for risk, and this influence may be ameliorated in the setting of RAD/ reversible obstructive disease either because of differences in inflammatory response as described above or increased lung plasticity in the setting of reversible obstructive disease [18].
We found that patients 65 years of age or younger had higher rates of toxicity than older patients, whereas prior studies have shown either an increased risk with increasing age or no relationship [9,13-14]. Since these patients were not treated in the setting of a prospective clinical trial, it is possible that this finding is the result of treatment bias. It is also possible that this unexpected finding is related to our institutional treatment approach of split course therapy, since we have noted in previous publications that our approach is much better tolerated by elderly patients and those with significant medical comorbidities than standard protocols[15-16]. It is possible that older patients are less able to mount a robust TH1 response to noxious stimuli and that this might lead to lower TGF beta and other cytokine levels during and after therapy, resulting in lower rates of subsequent toxicity, but this hypothesis has not been proven, and our lack of TGF beta levels precludes an assessment in this study [42].
Tumor location has been shown to be predictive of toxicity in some but not all prior studies, with some showing no relationship (for left versus right, or for individual lobes) and others showing increased toxicity with right-sided or lower lobe tumors [22,43]. We found a borderline statistically significant increase in toxicity for left-sided tumors, but there was no difference in severe toxicity based on tumor location.
It is possible that the introduction of planned radiotherapy treatment breaks in our regimen may influence our patterns of toxicity. As noted in our prior publications, our regimen has an overall favorable toxicity profile, but most of the reduction in toxicity probably relates to reductions in acute hematologic toxicity and esophagitis (resulting in very little weight loss during treatment and few unplanned treatment breaks)[15- 16]. Since neither RP nor PF represent early toxicity events, it is unlikely that the increase in overall radiation therapy treatment time (from approximately 6-7 weeks with a traditional approach to 12 weeks with our approach) would meaningfully influence the rate of these toxicities [44]. Therefore, we feel that the risks of our analysis can likely be generalized to patients treated with more traditional regimens.
The strengths of the current study are the homogeneity of the study population and the treatment regimen. The weaknesses our study include its retrospective nature, the fact that the patients being reviewed were not treated in the context of a clinical trial (introducing the possibility of selection bias and potential inhomogeneity in radiotherapy plan review and approval), and the lack of TGFbeta/ cytokine data. As mentioned previously, we will be reporting the results of our dosimetric analysis separately, and we will also be performing a separate analysis of the various chemotherapy regimen employed in this series.
Following treatment of locally advanced NSCLC with our institutional protocol of split course concurrent chemoirradiation, we found that asthma/RAD and smoking during and /or after definitive treatment reduced rates of toxicity, while a history of moderate to severe COPD (by GOLD criteria) increased the risk of toxicity. We also found that multiple baseline measures of pulmonary function were predictive of toxicity, and that the use of steroid controller trended toward lower rates of toxicity. These findings should be further validated in the context of a prospective trial.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
