
Research Article | DOI: https://doi.org/10.31579/2641-0419/260
1 Bayelsa Specialist Hospital, Yenagoa
2 Niger Delta University Teaching Hospital, Okolobiri.
3 University of Port Harcourt Teaching Hospital, Port Harcourt
*Corresponding Author: Emmanuel Auchi Edafe, Bayelsa Specialist Hospital, Yenagoa.
Citation: Emmanuel A. Edafe., Maclean R. Akpa (2022). The Heart and Vessels Foreign Bodies. A 3-Year Review. J. Clinical Cardiology and Cardiovascular Interventions, 5(5); DOI:10.31579/2641-0419/260
Copyright: © 2022 Emmanuel Auchi Edafe, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 March 2022 | Accepted: 11 April 2022 | Published: 18 April 2022
Keywords: foreign body; heart; vessels; the percutaneous retrieval; intravascular foreign bodies
Introduction
Foreign bodies in the heart and vessels are rare. They are usually iatrogenic. They get to the heart through different ways. They may cause serous complication including embolism and arrhythmias. They can could be diagnosed with X-ray, computerized tomography, and echocardiography. They are removed by endovascular percutaneous, surgical or conservative. In this four-year review, we analyzed identify and analyzed the treatment of foreign body referred to the Bayelsa Specialist Hospital.
Methods
We searched the cardiac catherization records of the hospitals and identify 11 foreign bodies referred for the period of 1st January 2018 and 30st April 2021. The site, etiology, clinical presentation, symptoms, complications and management modality, and outcome were noted.
Results
The patients mean age was 57. There were more women than men 8 versus 4 [P < 0.002]. The most common foreign bodies were parts of inferior vena cava filters and devices. Foreign bodies in the heart were symptomatic in 76% of patients. Right atrial chamber, inferior and superior vena-cava were occupied more often. A total of 78% presented within the first 24 hours. A majority of foreign bodies reached the heart by migration. There was no mortality among those treated with endovascular percutaneous therapy. All those treated in our center were by endovascular percutaneous and conservative therapy.
Conclusion
Foreign bodies in the heart and vessels may be asymptomatic or present with a wide variety of symptoms. Health care providers should be aware of this rare event and act fast dealing with it.
Foreign bodies in the heart and vessels are rare.[1] They are usually iatrogenic.[1] Embolism and arrhythmias may be part of the complications. [2,3] They can be diagnosed with X-ray, computerized tomography and echocardiography. They are removed by endovascular percutaneous or surgical methods. Conservative management is also an option. [3,4]
The objective of the study is to describe the pattern of treatment of foreign bodies referred to the Bayelsa Specialist Hospital.
It is retrospective study. We searched the cardiac catherization records of the hospital and identified 11 foreign bodies seen between 1st January 2018 and 30th April 2021. The site, etiology, clinical presentation, complications and management modalities and outcome were noted. Data were analyzed using SPSS version 25
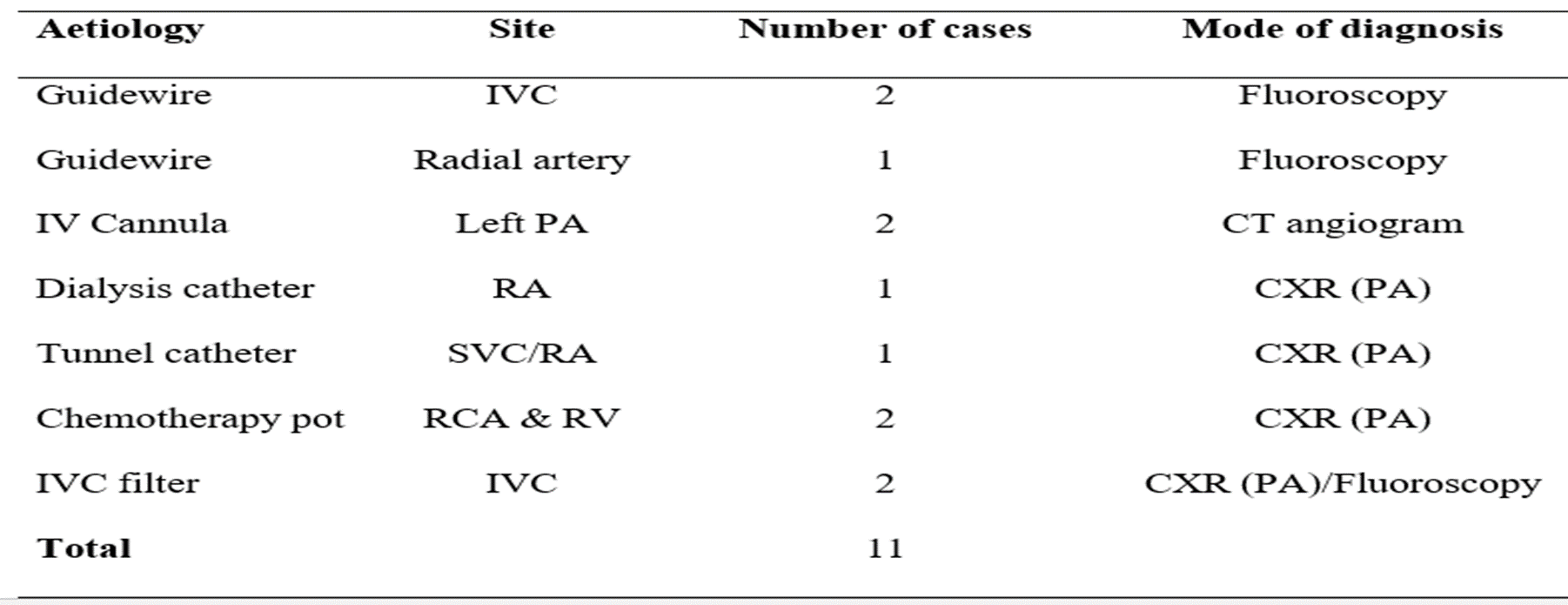
The patients mean age was 58. There were more women than men (7 versus 4 respectively). The most common foreign bodies were found in SVC, RA and inferior vena cava. [see Table 1]

The mode of diagnosis of the heart and vessels foreign bodies are Computed Tomography, fluoroscopy and X-ray. This is shown in Table 2.
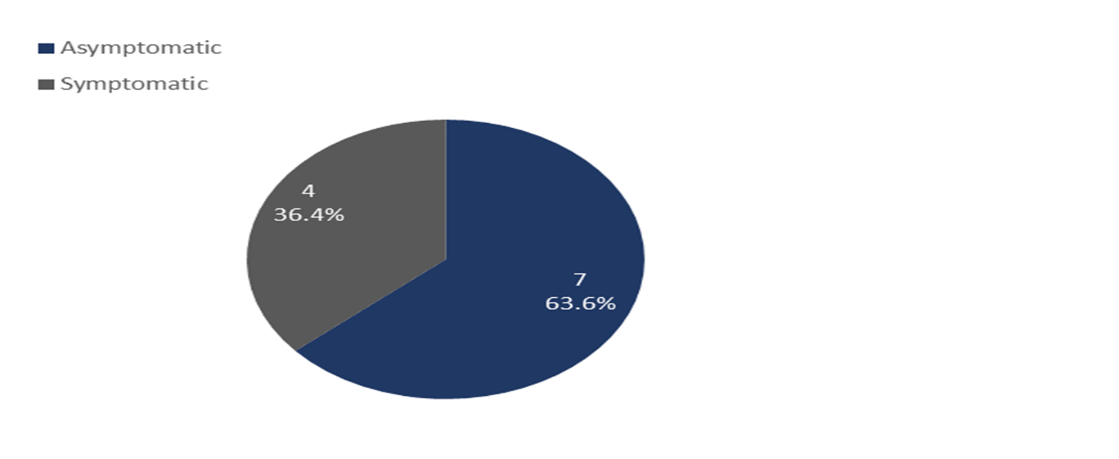
Foreign bodies in the heart were symptomatic in 36.4% [4 of the 11 patients]. The documented symptoms included palpitation, intermittent chest pain. Right atrial chamber, inferior and superior vena cava were more sites. This is probably due to the source of migration of foreign bodies from femoral vein, jugular vein or the subclavian vein. [See figure 1]
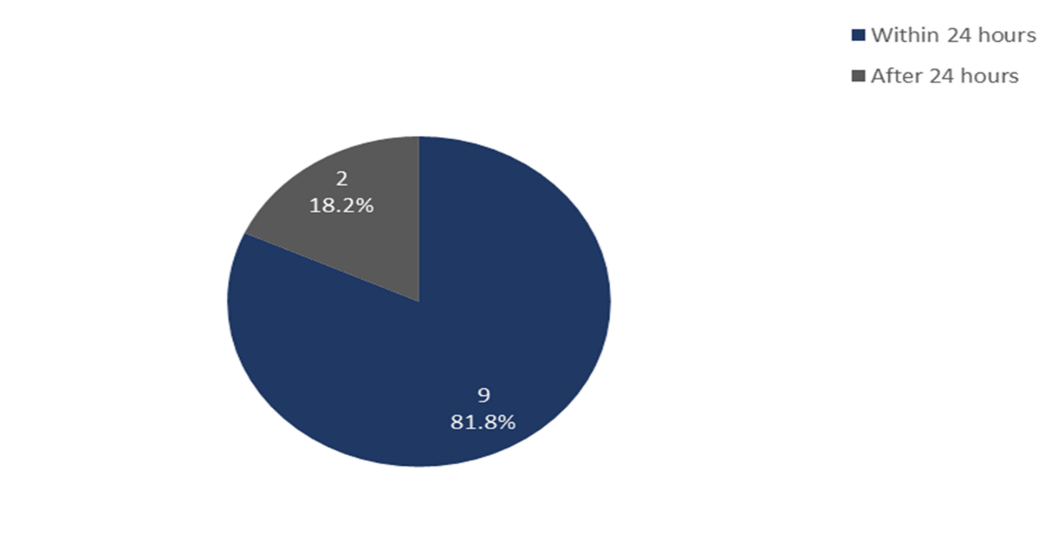
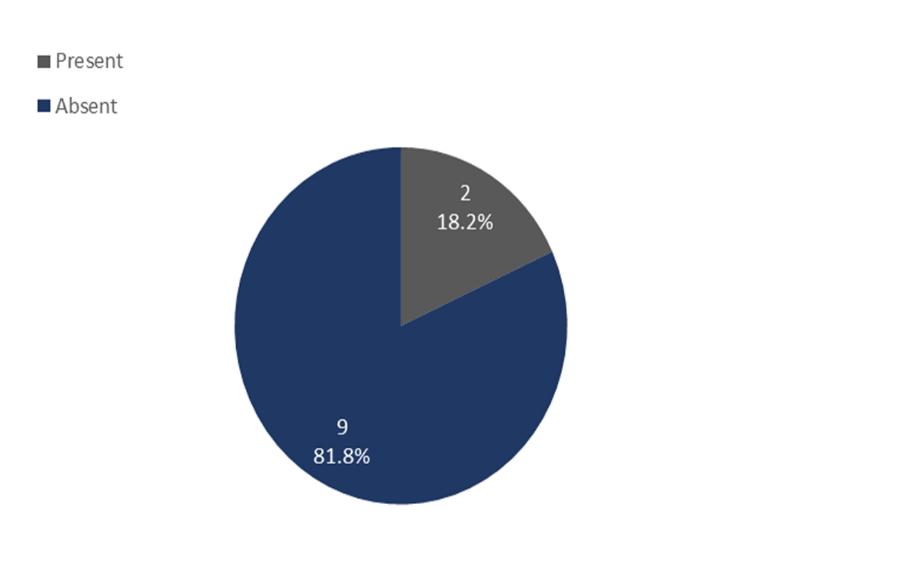
A total of 81.8 %[9 out of the 11 patients] presented within the first 24 hours. A majority of foreign bodies reached the heart by migration. There was no mortality among those treated with endovascular percutaneous therapy. All those treated in our center were by endovascular percutaneous and conservative therapy. The complication recorded were atrial and ventricular ectopics and non-sustained ventricular tachycardia on Electrocardiography. [see figure 2 and 3]
Nine patients received endovascular treatment while 2 were managed conservatively. They endovascular therapy with snare retrieval devices. The nine were successfully treated. There were no complications.
The two patients with fractured cannulas were managed conservatively, they were asymptomatic. The fracture cannulas were in the distal pulmonary artery. They were diagnosed with computed tomography but cardiac catherization laboratory did not identified the fractured part of the cannulas. [see figure 4 and 5]
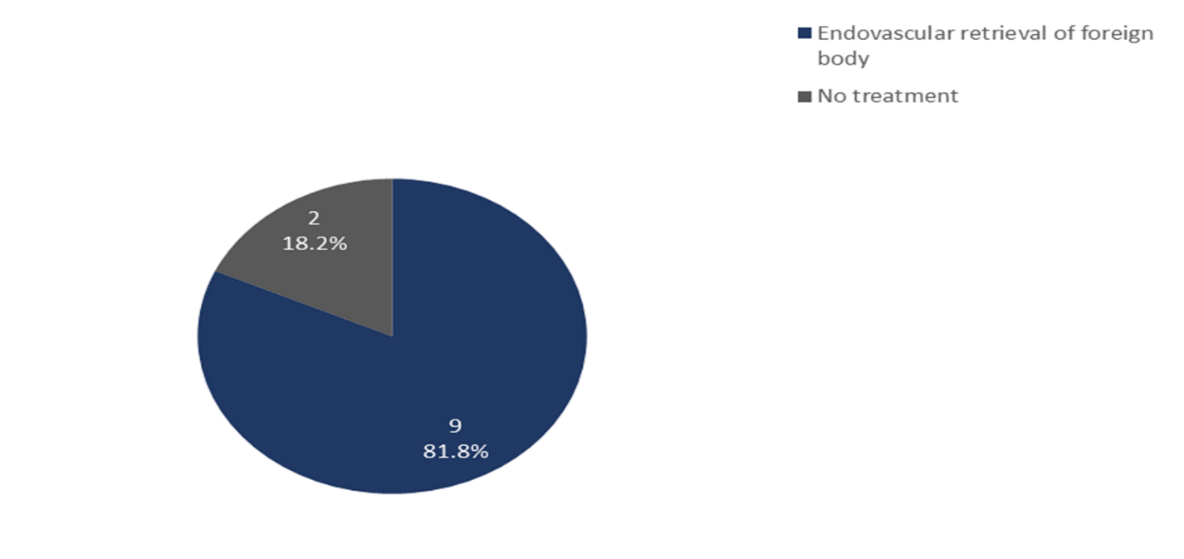
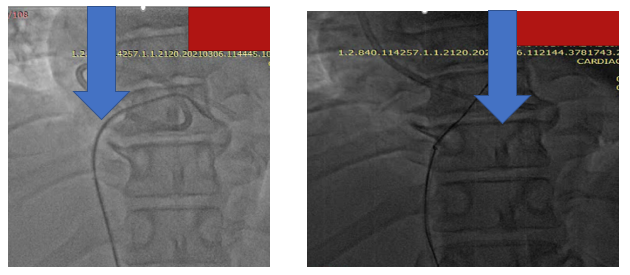

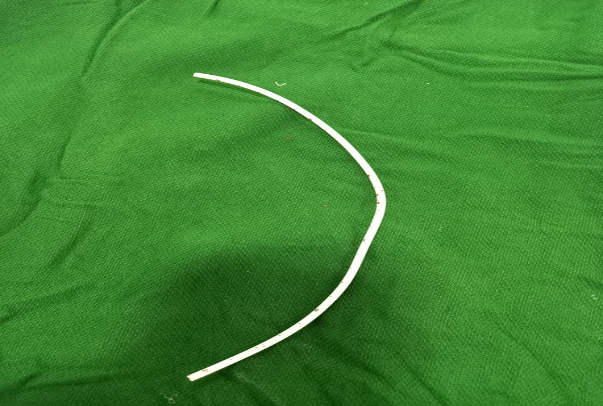
Figure 5: foreign body retrieval
The management of foreign bodies in the heart should be individualized. [3-4] Symptomatic foreign bodies should be removed by endovascular or surgical therapy.[5] In our review, we retrieved 9 of the 11 patients. The remaining 2 unretrieved were conservatively managed after a team review. Asymptomatic foreign bodies diagnosed immediately after the injury with associated risk factors should also be removed should be removed by endovascular or surgical therapy.[5] Asymptomatic foreign bodies that are incidental findings may be managed conservatively or removed.
Classification of heart and vessel foreign bodies
There is no uniform classification of heart and vessel foreign bodies. However, we suggest that FB can be grouped as venous and arterial foreign bodies. Venous foreign bodies migrate and embolize to the right atrium, right ventricle and pulmonary artery. Arterial foreign bodies follow the direction of blood flow. Limb arterial foreign bodies embolize to the end of the extremities. Our review had one left radial artery that occurred during radial puncture. The fragmented guidewire embolized to the distal radial artery. It was retrieved through the femoral route.
The left ventricle can also harbor foreign bodies from penetrating injuries, or fragmented part of wires or catheter during percutaneous procedures within the cavity. Ayx and his colleagues in a review of the interventional removal of intravascular Medical Devices noted that a guide wire could not be extracted as it was already adhered with the vessel wall.[6] Our review noted two fragmented intravenous cannulas that migrated to the distal pulmonary artery. They were managed conservatively.
Sites of heart and vessel foreign bodies
Surov at al in a systemic review of intravascular embolization of venous catheter-causes, clinical signs, and management the sites of catheter fragments following embolization were the superior vena cava or peripheral veins (15.4%), the right atrium (27.6%), right ventricle (22%), and pulmonary arteries (35%).[7] Our study also found SVC, IVC, and RA as more common sites of venous foreign bodies.
The present study found two guidewires were in the IVC; one guide wire is found in the distal left radial artery; two cannulas were found in the in the distal pulmonary arteries. A fractured dialysis catheter embolized to the right atrium. Another fractured tunnel catheter migrated to the right atrium and right ventricle. Two chemotherapy pots embolized to the RA. Another two IVC filter migrated to proximal IVC.
Clinical presentation of foreign bodies
A systemic review by Soruv et al found clinical signs of catheter embolization to include catheter malfunction (56.3%), arrhythmia (13%), pulmonary symptoms (4.7%), and septic syndromes (1.8%), and 24.2% of cases were asymptomatic.[7] The symptoms may include thrombosis, atrial and ventricular arrythmias, infections and depressive-anxiety manifestation. Other complication may include endocarditis. The present study found 4 (36.4%) symptomatic and 7 (63.6%) were asymptomatic. Among the symptoms in our study were atrial and ventricular ectopics and non-sustained ventricular tachycardia.
Foreign bodies in the heart and vessels may be asymptomatic or symptomatic.
They are usually iatrogenic and should be referred for appropriate management. Bulker and lengthier devices may result in more severe complications.
SVC, Superior vena-cava
RA, right atrium
RV, right ventricle
IVC, inferior venacava
FB, foreign body
Management of Bayelsa Specialist Hospital for the kind coorperation during the data collection.
EAE review the patients at admission and confirmed the diagnosis. EAE performed the endovascular procedure, drafted the work and collected the data. RMA participated in the data collection and analysis. The authors read and approved the final manuscript.
None.
Availability of data and materials
All data generated or analyzed during this review are included in this
publication.
Ethics approval and consent to participate
Ethical approval was sort from the hospital ethical committee. Consent was sort from the patients that the data will be used for research without their names.
Consent for publication
A written informed consent of all details/images or videos relating to the
patient for publication was obtained from the patients
Competing interests
The authors declare that they have no competing interests.
It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,

Dear Maria Emerson, Editorial Coordinator of International Journal of Clinical Case Reports and Reviews, What distinguishes International Journal of Clinical Case Report and Review is not only the scientific rigor of its publications, but the intellectual climate in which research is evaluated. The submission process is refreshingly free of unnecessary formal barriers and bureaucratic rituals that often complicate academic publishing without adding real value. The peer-review system is demanding yet constructive, guided by genuine scientific dialogue rather than hierarchical or authoritarian attitudes. Reviewers act as collaborators in improving the manuscript, not as gatekeepers imposing arbitrary standards. This journal offers a rare balance: high methodological standards combined with a respectful, transparent, and supportive editorial approach. In an era where publishing can feel more burdensome than research itself, this platform restores the original purpose of peer review — to refine ideas, not to obstruct them Prof. Perlat Kapisyzi, FCCP PULMONOLOGIST AND THORACIC IMAGING.
