AUCTORES
Globalize your Research

case report | DOI: https://doi.org/10.31579/2690-1897/247
President of all nations Morning star hospital, Enayam Thoppu, Kanyakumari District, India.
*Corresponding Author: Ramachandran Muthiah, President of all nations Morning star hospital, Enayam Thoppu, Kanyakumari District, India.
Citation: Ramachandran Muthiah, (2025), Surgical Aspects of Brain Abscess – A Case Report, J, Surgical Case Reports and Images, 8(4); DOI:10.31579/2690-1897/247
Copyright: © 2025, Ramachandran Muthiah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 March 2025 | Accepted: 25 March 2025 | Published: 03 April 2025
Keywords: tetralogy of fallot; vegetation; brain abscess; four component therapy; surgical aspiration
Aim: To report a case of solitary, parietal lobe abscess in a boy, aged 16 years in Tetralogy of Fallot.
Introduction: Infective endocarditis is a serious and fatal complication in congenital heart disease. Following bacterial endocarditis, ventricular septal defect (VSD) and Tetralogy of Fallot (TOF) have less morbidity and higher survival rate in children. Neurological complications were recognized in 20 % of cases and brain abscess is a serious infection of brain parenchyma as a result of seeding of infective pathogens in the shunted blood from the right side of the heart.
Case report: A 16-year-old boy had Tetralogy of Fallot, presented with altered sensorium of sudden onset. Echocardiography revealed a large vegetation, attached to the ventricular septum and a large VSD with overriding of aorta. CT brain revealed a large abscess cavity in the parietal lobe, which was evacuated by aspiration and treated with antibiotics.
Conclusion: Any patient presented with altered sensorium in cyanotic congenital heart disease must be evaluated with CT scanning for brain abscess and also check hematocrit to rule out hyperviscosity syndrome. Lumbar puncture has been considered hazardous in patients with brain abscess and usually performed under a strong suspicion of meningitis or ventriculitis in the absence of increased intracranial pressure.
Cyanotic congenital heart disease is characterized by intracardiac right-to-left shunting of unsaturated blood and its distribution into the systemic circulation resulting in arterial hypoxaemia, leading to pulmonary vasoconstriction, altered acid base status, polycythaemia, coagulopathy, infective endocarditis (IE) and brain abscess due to increased risk of paradoxical embolism. Cyanotic heart disease accounts for 12.8-69.4 % of all cases of brain abscess with the incidence being higher in children [1],[2]. The risk of brain abscess complicating cyanotic CHD (congenital heart disease) is inconstant, but is more common after two years of age and increases consistently until the age of 12 years. Of all the patients with brain abscess and cyanotic congenital heart disease, TOF (Tetralogy of Fallot) is the most common in association (13-70 %) of cases [3-7]. Infective endocarditis typically presents more insidiously in patients with congenital heart disease. The risk of infective endocarditis in cyanotic CHD is more than six times the risk compared to those in acyanotic CHD. Patients with congenital heart disease have structural changes that create turbulence and shear force in blood blow that disrupts the endocardium, exposing the subendocardial collagen and extracellular matrix. The resultant inflammation causes endothelial cells to express β1 integrins, which bind circulating fibronectin to the endothelial surface and promote scar formation. During the healing process, production of tissue factor, deposition of fibrin, and platelet adherence lead to hemostasis and pathogenic organisms may settle in and infect the endocardium in these scarred areas. With sequestration and limited blood supply to a damaged area, formation of vegetation and / or abscess may occur. These friable vegetations have the capability of causing emboli, which may result distal abscess formation, especially in the brain and so this case had been reported.
A 16-year-old cyanotic male was admitted with altered sensorium in the intensive care unit. He was diagnosed as Tetralogy of Fallot and advised corrective surgery earlier. He was afebrile and his pulse rate was 64 bpm and blood pressure 100/60 mmHg. He had headache, vomiting episodes and stiff neck for the past 3 days. Blood chemistry revealed normal. ECG and X-ray chest as in Figure 1 (boot-shaped heart) were consistent with Tetralogy of Fallot. Physical examination revealed uniform central cyanosis with clubbing, 2/6 systolic murmur in the left second intercostal space and a single second sound. Echocardiography revealed a non-restrictive, large, malaligned VSD (ventricular septal defect), biventricular aorta as shown in Figure 2. A large vegetation was attached to the crest of interventricular septum (IVS) as in Figures 3 and 4.
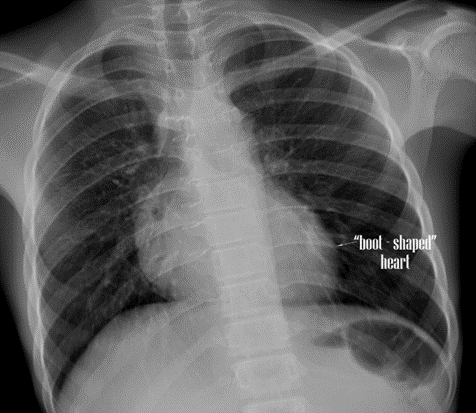
Figure 1: X-ray chest PA ( Postero-anterior) view showing the “boot-shaped heart” (arrow) of tetralogy of Fallot with oligemic lung fields in a 16 year old boy.

Figure 2: showing the large, malaligned VSD (ventricular septal defect) of Tetralogy of Fallot in a 16-year-old boy.

Figure 3: showing “the vegetation” (arrow) attached to the crest of IVS (interventricular septum) in a 16 –year old boy with Tetralogy of Fallot.

Figure 4: showing “the vegetation” (arrow) seen across the VSD (ventricular septal defect) in a 16 –year old boy with Tetralogy of Fallot.

Figure 5: CT brain showing the large abscess cavity in the parietal lobe with mild midline shift in a 16 –year old boy with Tetralogy of Fallot. Upper arrow showing the Rim (capsule) and the lower arrow showing the abscess cavity.

Figure 6: CT brain showing the large abscess cavity in the parietal lobe with “ daughter abscess” in the lower part (lowest arrow) with moderate midline shift in a 16 –year old boy with Tetralogy of Fallot.

Figure 7: CT brain showing the large abscess cavity in the parietal lobe with small “daughter abscess” in the upper part (right arrow) in a 16 –year old boy with Tetralogy of Fallot.
CT (computed tomography) brain revealed a large abscess cavity in the parietal region as in Figures 5, 6 and 7. The abscess was aspirated via burr-hole and cultures were found to be negative. He was given ceftriaxone 1g IV twice daily, amickacin 500 mg IV twice daily with tablet phenytoin sodium 100 mg twice daily for 2 weeks. He was symptom free and advised periodic follow up. On 1 year follow up, the patient was asymptomatic without any sequelae and advised corrective surgery for the cardiac anomaly at the earliest.
3. Discussion
Review of literature
Rushani and colleagues found that 34 % of children with infective endocarditis had cyanotic CHD [8]. Elder and Baltimore found that infective endocarditis represented 0.05 to 0.12 per 1000 pediatric admissions. Tetralogy of Fallot (TOF) was described in 1888 by the French physician Etienne-Louis Arthur Fallot [9]. In 1814, Farre [10] discussed a case of tetralogy of Fallot in a boy aged 9 years who died of brain abscess. Lallemand Louis and Berthody [11] described similar cases and in 1880, Ballet reviewed the literature of it. Abbott and her collaborators [12] reported two cases in 1923 and Rabinowitz and associates [13] were the first to report a case with correct antemortem diagnosis in 1932. Weehslar and Kaplan [14] described two cases in 1940.
Etiopathogenesis
TOF accounts for 10 % of all cases of congenital heart disease [15] and the incidence of brain abscess in population with congenital heart disease varies from 5 to 18.7 % [16]. In Fallot’s tetrad, Bing and associates [17] have shown that the shunting from right-to-left occurs in the absence of failure, owing to the overriding of aorta. When a reversal of flow is said to occur, favoring paradoxical embolism and paradoxical brain abscess stands second only to bacterial endocarditis. Acute infective endocarditis is a tumultuous, destructive infection frequently involving a highly virulent organism such as staphylococcus or pseudomonas. Staphylococcus aureus is pervasive, with fibronectin binding protein on its surface. When integrins are exposed, they provide a self-adhesive surface for circulating staphylococci which may also infect normal undamaged endocardium and once adherent, staphylococcus aureus internalizes and escapes host defences. Subacute infective endocarditis is “benign” with a typically more indolent course, often more than 6 weeks, and usually involves a less virulent organism such as streptococci infecting an anatomically damaged heart. Some viridans group streptococci have a type 1 fimbrial subunit that is a major adhesive protein to fibrin platelet aggregates. Pulmonary circulation represents a potential filtering apparatus for systemic bacterial pathogens. In patients with right-to-left shunts, absence of pulmonary phagocytic clearance of pathogens can occur and the ischemic injury from hypoxaemia and polycythaemia, resulting low perfusion areas (microinfarcts) in the brain which may act as a nidus for infection [18]. In the development of brain abscess, inoculation of an organism is required into the brain parenchyma in an area of devitalized brain tissue or in a region with poor microcirculation and the seeded microorganisms can sustain growth and multiply to form abscess. Altered blood brain barrier permeability also play a role and infections from any systemic source may lead to bacteremia and subsequent spread to brain parenchyma even in the absence of cyanotic heart disease. Brain abscess begins with a localized area of inflammatory change referred to as cerebritis. This early stage of infection is characterized by increased blood vessel permeability without angiogenesis. When unrecognized, this process will progress to an immature capsular stage and then to brain abscess, a condition defined by an area of parenchymal infection containing pus encapsulated by a vascularized membrane. Histologically, there are four stages in brain abscess formation: early cerebritis (day 1-3), late cerebritis (day 4-9), early encapsulation (day 10-13) and late capsule stage (> 14 days) [19]. About 2 weeks are required for encapsulation, which is usually less complete on medial or ventricular side due to poor vascular supply [20]. The brain abscess capsule serves to prevent the infective process from becoming generalized and it also creates within it an inflammatory “soup” that may impede resolution of the infection. The mode of entry of organism could be by contiguous (primary dental, sinus, ear infections, or mastoiditis) spread (14 to 58 %), hematogenous (endocarditis, pulmonary infections such as pneumonia, empyema and abscess) dissemination (9 to 43%) from a distant site as investigated by Warrington in 1918 [21] or following trauma and invasive neurosurgical procedures (3 to 18 %). The incidence of brain abscesses is about 8 % of intracranial masses in developing countries, whereas, in Western countries, the incidence is about 1-2% [22]. The predisposing factors of brain abscess are shown in Table 1.
Congenital heart disease with a right-to-left shunt [23] Infections of middle ear, mastoid, paranasal sinuses, orbit, face, scalp, penetrating skull injury and comminuted skull fracture Intracranial surgery including insertion of ventriculo-peritonial shunts Abnormal immune functions [24] |
Table 1: showing the predisposing factors of brain abscess
Several predisposing factors are casually related, but in `14-25 % of patients, no cause can be found [25],[26]. A single organism is isolated in majority of bacterial brain abscess. Anaerobic streptococci are most common agents in cyanotic heart disease with brain abscess. However, isolation of multiple pathogens from abscess materials is not uncommon (4-23 %) [27],[28]. Cultures are negative in 16-68 % of brain abscess with cyanotic heart disease [29]. Administration of antibiotics prior to the collection of abscess material is often cited as the explanation for sterile culture. The abscess drained within 3 days of antibiotic administration had much greater yield than otherwise (84 % and 32 % respectively) [30]. Bacteroides fragilis and peptostreptococcus are the most common anaerobic organisms isolated [31]. Organisms vary significantly with the etiology of abscess as shown in Table 2 [32].
Source Most commonly cultured organisms |
Paranasal sinus infection Streptococcus spp Staphylococcus spp Enterobacteriaceae (especially Hemophilus spp, , Pseudomonas aeruginosa)
Otogenic infection Proteus mirabilis Streptococcus milleri group organisms Streptococcus pneumoniae Staphylococcus aureus
Dental infection Streptococcus spp Bacteroides fragilis
Traumatic brain injury Staphylococcus aureus Staphylococcus epidermidis Enterobacteriacea (most Commonly P.aeruginosa, Enterobacter spp)
Neurosurgical procedure Staphylococcus aureus Staphylococcus epidermidis Pseudomonas aeruginosa Propionibacterium acnes Streptococcus spp.
Hematogenous spread Staphylococcus aureus Streptococcus viridans Klebsiella pneumoniae
|
Table 2: showing the varying organisms with the etiology of abscess.
Individuals with AIDS having brain abscess are more likely to have multiple abscesses and tuberculous abscess. Toxoplasma encephalitis is the most common multifocal infectious process encountered in advanced HIV and this population is more susceptible to intracranial infections from Listeria, Cryptococcus, and Nocardia [33]. Fungal brain abscess mostly related to Aspergillus and other species including candida are common in organ transplant patients and immunocompromise raises the risk of CNS infection with an incidence as high as 37.5 %. Moyamoya disease, a vaso-occlusive disease of cerebral blood vessels with a number of collaterals at the base of brain giving a "smoke of puff " (“moyamoya" in Japanese) is rarely associated with TOF and presents with CNS involvement such as stroke and seizures [34] and may produce abscess in the brain. Abscess can occur in any location of brain, which is closely associated with source [35]. Otogenic abscess occurs almost exclusively in the temporal lobe and cerebellum [36], while abscess associated with sinus infection is predominantly frontal [37],[38]. A significant proportion of individuals develop multiple abscesses (9.3-28%) [39],[40],[41].
Echocardiographic features
The four components of TOF are ventricular septal defect (VSD), aortic override, right ventricular outflow tract obstruction and right ventricular hypertrophy. In unrepaired TOF, pathophysiology depends on the degree of RVOT obstruction. When obstruction of right ventricular outflow is mild to moderate and a fairly balanced shunt operates across VSD and the patient may not be cyanotic , called as “acyanotic” or “pink” tetralogy of Fallot. The patient may remain relatively asymptomatic until the balance between pulmonary and systemic circulation is disturbed. Echocardiography plays a key role in the diagnosis of infective endocarditis (IE) in TOF. Vegetation may occur on pulmonary and tricuspid valves [42] and a large vegetation occluding the VSD had been reported [43]. In this patient, a large vegetation attached to the crest of interventricular septum was shown in Figures 3 and 4.
CT imaging
Brain abscess is an encapsulated inflammation and can be easily diagnosed by CT scan. The CT appearance of an abscess is that of a well-defined hypodense area showing ring enhancement and accompanied by extensive perifocal edema and mass effect. The ring enhancement on the CT scan surrounding a central necrotic cavity as in Figure 5 is an abscess. The appearance of enhancing rim, the capsule of the abscess enhances and it is variable. The rim is formed probably by collagen and inflammation due to free radicals and micro hemorrhages in the abscess. The abscess tends to grow towards white matter, away from the better vascularized grey matter, with thinning of the medial wall. The preferential deposits of collagen on the outer edge of the abscess is thought to be due to the vascularization of grey matter. The zone of inflammation is significantly thicker in tuberculous as compared to pyogenic abscess. The neuroimaging features of brain abscess vary with lesion stage as shown in Table 3. During the cerebritis stage (local suppurative encephalitis or immature abscess), ring enhancement may be absent or incomplete. Abscesses with a more nodular rim are often mistaken for neoplasm. Brain abscesses tend to have a smooth, thin-walled capsule and it is more irregular in tumors. In contrast to tumor, the abscess rim is typically thicker near the cortex and thinnest near the ependyma. Early capsule stage is characterized by formation of a distinct collagenous capsule, which is well delineated, relatively thin, uniform and continuous. The uniformely enhancing capsule is typical of a mature abscess. The abscess gradually shrink, peripheral edema diminishes and then disappears in the late capsule stage.
| Stages | CT appearance |
Early cerebritis
Late cerebritis
Early capsule
Late capsule | May be invisible Poorly marginated cortical or subcortical hypodensity with mass effect with little or absence of enhancement An ill-defined area of low density on plain CT corresponds to developing necrotic center in the cerebritis stage
irregular ring-enhancing lesion with a hypodense center, better defined than early cerebritis
well-defined rim-enhancing mass, an outer hypodense and inner hyperdense rim (double rim sign) is seen in most cases. A slightly hyperdense, faint ring is seen surrounding a necrotic hypodense center [44]
Rim-enhancing lesion with thickened capsule and diminished hypodense central cavity. The capsule is seen as a ring in plain CT |
Table 3: The CT features of brain abscess according to the stages of development
The apparent budding of smaller, ‘daughter’ lesion from the main mass is called as “daughter abscess”. In about 50% of cases, the medial wall of an abscess is thinner than the lateral one and is thought to be due to the relatively poor vascular supply of the white matter. This explains the tendency of abscess to rupture into the ventricles and the development of secondary abscesses (daughter abscess) medially [45] may be seen near the primary lesion as in Figures 6 and 7. In deep seated, multiloculated and periventricular abscesses, a reduction of 1 mm in the distance between the ventricle and brain abscess wall increases the rupture rate by 10% [46]. Smooth, < 5>
As reported by Landriel, et al [48], brain abscesses were solitary in 77.7% of the subjects and multiple (22.3%) abscesses are more common in immunocompromised children and infective endocarditis [49]. The temperoparietal region was the most commonly affected location in a study carried out by Cavusoglu, et al [50]. In children, the most common location was in the parietal region (55%), frontal (28%), temporal (13%)
and occipital (4%). The location of brain abscess as stated by Brook [51] was frontal lobe (47.1%), parietal (29.4%), temporal (13.7%) and occipital (9.8%). MRI has also proven to detect small, multiple abscesses and may render superior images of posterior fossa location and more sensitive to distinguish cerebritis from necrosis [52], but not better than CT in distinguishing abscesses from neoplasms and the diffusion-weighted imaging can aid in this distinction [53] as hypointense abscess capsule on T2-weighted sequence may allow for this differentiation and the surrounding edema is apparent whereas in T1-weighted image, the capsule enhances and the interior of the abscess is hypointense. In T2-weighted images, the wall of the abscess is dark and it is bright in neoplasms. MRS (Magnetic resonance spectroscopy) appears to be useful in the diagnosis of abscesses arising from anaerobic infections because these species produce lactate and acetate, which are readily apparent on MRS and rarely found within tumor tissue [54]. Practically, all abscesses > 1 cm produce positive scans. Thus, CT scan appears to be adequate in most cases of brain abscess, but in very small miliary abscesses and brain stem abscess in which MRI with specialized sequence or MRS is indicated.
Management
The first reference to brain abscess is attributed to Hippocrates in the fifth century B.C [55]. Sir Williams MacEwen was called as the "father' of modern brain abscess management for the publication of his famous monograph Pyogenic Infective Diseases of the Brain and Spinal cord in 1893. The treatment of brain abscess has been a challenge. The basic principle of treatment is the selection of appropriate antibiotics with or without aspiration.
Medical therapy
Small brain abscesses have been treated empirically with antibiotics [56]. Heineman and colleagues became the first to report the successful medical management of a brain abscess in 1971 [57]. Medical therapy alone can be considered in patients with a lesion in the cerebritis stage since they are much more likely to respond to antibiotic therapy because of lack of a capsule [58] and also for walled off, but<2>
Hyperbaric oxygen therapy (HBO2 or HBOT)
It is indicated as a primary and adjunct treatment to reduce intracranial pressure and high partial pressure of oxygen act as a bactericide and thus inhibit the anaerobic flora common in brain abscess. It optimizes the immune function, enhancing the host defence mechanisms and it has been found to be of benefit when brain abscess is concomitant with cranial osteomyelitis.. It also increases the stem cell production and up-regulation of VEGF which aid in the healing and recovery process [69].
Anti-inflammatory agents
The glial cell activation in brain abscess is through parenchymal microglia and astrocytes. Activated microglia has the potential to influence the type and extent of antibacterial adaptive immune response through upregulation of MHC class II and costimulatory molecule expression. The control release of proinflammatory mediators may damage the surrounding brain parenchyma [70] and the cytokines IL-1 and TNF-α establish an effective antibacterial response in the CNS parenchyma. Recent studies support persistent immune activation in brain abscess with elevated levels of IL-1, TNF-α and macrophage inflammatory protein-2 (MIP-2), detected 14 to 21 days following staphylococcus aureus exposure. Interventions with anti-inflammatory agents subsequent to sufficient bacterial neutralization may be an effective strategy to minimize the damage in the surrounding brain parenchyma during the course of brain abscess development, leading to improvements in cognition and neurological outcome [71]. However, if coagulation abnormalities are present, especially in cyanotic CHD, nonsteroidal anti-inflammatory drugs should be avoided, platelet concentrate should be available perioperatively [72] and when the hematocrit > 65% requires phlebotomy and adequate hydration to maintain intravascular volume.
Role of steroids
Corticosteroids play a role as an adjunctive therapy to control cerebral edema in patients with potentially life-threatening complications such as impending cerebral herniation. Corticosteroids are used when a significant mass effect is visible on imaging and the patient’s mental status is depressed, but had some adverse effects to retard the encapsulation process [73],[74], increase necrosis, reduce antibiotic penetration (polar antibiotics such as benzyl penicillin) into the abscess, increase the risk of ventricular rupture, and decrease the enhancement of abscess wall on CT due to contrast reduction as inflammation subsides [75]. The tissue concentrations of more lipophilic substances, such as metronidazole, were not affected by concomitant corticosteroid therapy [76] and it should be the part of antibiotic regimen. The corticosteroid of choice for reducing the intracranial pressure is dexamethasone and it may decrease inflammation by suppressing the migration of polymorphonuclear leukocytes and reversing increased capillary permeability. When used to reduce the cerebral edema, therapy should be of short duration and high-dose corticosteroid therapy (IV dexamethasone 8 mg every 8 hours) should be given and then tapered off after the patient’s condition has stabilized. Even though retrospective studies failed to show a beneficial effect of corticosteroids on outcome [77],[78], however, corticosteroids are given mostly to severely obtunded and comatose patients who are known to have a dismal prognosis [79],[80]. Severe brain abscess may necessitate further measures to reduce the increased intracranial pressure, such as osmotherapy (e.g. mannitol and moderate hyperventilation. Even though mannitol helps to decrease intracranial pressure, cerebral edema and ideal to reduce blood viscosity, it can cause severe dehydration, hypotension, tachycardia, acidosis and precipitate “tet spell”.
Surgical therapy
Surgery is the treatment of choice for most brain abscess to confirm the diagnosis, allow direct identification of the causative organism, and to decompress the abscess cavity. A number of surgical techniques have been developed to treat brain abscess over the last two centuries, range from the tube drainage methods of the past to modern computer-guided minimally invasive approaches for abscesses < 1>
Tube drainage as shown in Figure 8
It is the oldest surgical technique, entry into abscess cavity with a needle, followed by placement of tube into the cavity for postoperative drainage. Its advantages are spontaneous drainage of abscess contents, decompression of surrounding brain and minimize trauma to brain. Its mortality ranges from 30 t0 50% and complicated by tube obstruction.

Figure 8: (Following trephination of the skull, a tube is inserted into the brain abscess, allowing the abscess to drain spontaneously. The tube is secured to the scalp following closure, to obtain chronic external drainage of the abscess)
Marsupialization is shown in Figure 9

Figure 9: (A broad section of cortex overlying the abscess is removed, allowing the abscess cavity to communicate with the cortical surface of the brain. Gauze is sometimes packed into the cavity to prevent reaccumulation of the abscess)
Migration technique as shown in Figure 10 A, B and C.
It is a two stage technique described by Khan in 1937 as decompressive craniotomy to release the increased intracranial pressure, brain abscess tend to migrate towards the cranial opening and a 2nd procedure 3-4 days later as excision or drainage.

Figure 10: A (Khan technique – stage 1, calvarial bone over the abscess is removed)

Figure 10: B (Khan technique- migration of abscess. The abscess is allowed to migrate towards the surface)

Figure 10: C (Khan Technique- stage II- Several days later, the abscess is treated by direct excision or aspiration)
Excision
It is described by Kronlein in 1910, a complete removal of infectious process with immediate relief from mass effect and relay on existence of collagenous capsule for clear plane of dissection. The mortality of this technique is 20% and in multiloculated Nocardia abscess, the craniotomy with excision effects a cure.
Aspiration
It is described by Mayfield and Spurling in 1937, a simple evacuation and decompression of abscess contents. It can be performed via a burr-hole opening and a lesion in eloquent brain or deep lesion can be drained. It does not remove infection, but simply decompress the cavity and the abscess reaccumulation may need repeat aspiration or excision in 50 to 70% of cases. The loculated abscess may not be successfully treated by aspiration. Aspiration through a burr-hole is shown in Figure 11.

Figure 11: (The needle is inserted into the abscess cavity and the contents are aspirated)
Image-Guided Technique (Stereotactic Aspiration)
stereotaxis consists of assigning three-dimensional coordinates to any point within the brain and can be used in small abscesses or abscesses within deep or eloquent brain. Its mortality rate is 0-21% and the risk of hematoma 1-4%. Ultrasound-guided aspiration of brain abscess is shown in Figure 12.

Figure 12: (The opening in the calvaria is enlarged to accommodate the head of an ultrasound probe. The abscess is visualized, and a needle is directed into it in real time)
Endoscopic fenestration is shown in Figure 13

Figure 13: (Endoscopic fenestration was performed in Primary intraventricular abscess, showing encapsulated abscess (arrow) and adhesion to the ventricular wall)
Per operative picture during endoscopic third ventriculoscopic interventions, showing emergence of tubercular pus from the lesion as shown in Figure 14(b,c)


Figure 14: (b,c) showing the emergence of pus
Surgical drainage provides the most optimal therapy and the procedures used are aspiration through a burr-hole and complete excision after craniotomy. Needle aspiration is preferred and the most commonly used technique, often performed using a stereotactic procedure with a guidance of ultrasound or CT scanning [85], especially for deep-seated abscesses (brainstem, cerebellum and basal ganglia). Often, external drainage of the abscess through an intra-cavity catheter is recommended for abscesses > 3 cm in diameter. Total excision is preferred for solitary, superficial and well encapsulated abscesses. Abscess containing gas are resistant to antibiotics and are better treated with excision [86]. Brain abscess caused by Nocardia asteroids are multiloculated and excision must be performed to effect a cure [87] and may not be successfully treated by aspiration. Excision is also reserved for abscesses that enlarge after 2 weeks of antibiotic therapy or that fail to shrink after 3-4 weeks of antibiotics because of adhesions to the dura and also for posterior fossa abscesses, especially in the cerebellum, which may compress CSF pathways and thereby lead to dangerously high intracranial pressure and carry a mortality rate of 20 to 50 % [88]. The current recommendations are to drain these abscesses through a posterior fossa craniotomy and to perform CSF diversion through an external ventricular drain in patients with any radiologic signs of hydrocephalus. Excision should not be considered for
abscesses in the cerebritis stage, deep-seated abscesses in the eloquent areas and multiple abscesses. The “migration technique” described by Khan in 1937 [89] is a two-stage technique that included a decompressive craniotomy followed by a second procedure 3 to 4 days later for either excision or drainage of the abscess. He noted that when a craniotomy was performed for the relief of increased intracranial pressure, brain abscess tended to migrate toward the cranial opening. Neuroendoscopic technique
with free hand stereotaxy has also been practiced [90] and it has an additional advantage of more complete drainage and lavage, when compared to stereotactic aspiration [91]. It is suggested that irrigation of abscess cavity with antibiotic solution raises antibiotic levels and reduces the bacterial load, allowing the infectious process to resolve more quickly [92]. However, local administration of antibiotics is not routinely recommended because intravenous antibiotics used for brain abscess treatment penetrate the brain and abscess capsule, achieving therapeutic intracavitary levels [93]. Antibiotic irrigation may prove helpful in case of rupture of a brain abscess into the ventricle [94].
Five component therapeutic plan
The encapsulation of a brain abscess often is more complete on the cortical than on the ventricular side. Thus, brain abscess is more likely to rupture into the ventricles rather than laterally into the subarachnoid space. The intraventricular rupture of brain abscess (IVOBRA) results in severe headache, an increase of meningeal irritation, a rapidly deteriorating clinical condition, and an enhancement of the ventricular wall adjacent to the abscess often preceded IVOBRA [95]. Most authors proposed an aggressive approach with regard to its clinical prognosis. Zeidman, Geisler, and Olivi have proposed a five-component therapeutic plan [96], consisting of open craniotomy with debridgement of the abscess cavity, lavage of the ventricular system, ventricular drainage, intrathecal gentamycin, and intravenous administration of appropriate antibiotics. However, the role of intrathecal antibiotics is disputed [97]. Seizure is a long-term risk for upto 30-50% of patients suffering from brain abscess [98]. The hypo-dense areas surrounding the abscess cavity are thought to cause epileptic activity and it is mainly related to scars after excision rather than with aspiration. Antiepileptic medication was advised in all cases and continued for at least 2 years and then slowly withdrawn when the EEG become normal and the patient is seizure free for at least 2 years after surgery. Legg advocated anticonvulsant therapy for 5 years to all patients with cerebral abscess [99]. Seizures are initial presentation of brain abscess up to 35% of cases and should be controlled with intravenous benzodiazepines such as lorazepam or midazolam or fosphenytoin. For the prevention of further seizures, carbamazepine is recommended, in addition to phenytoin. The risk of recurrence is 10-50%. To prevent recurrence of the abscess, the source of infection should be treated surgically or medically [100]. Correction of cardiac anomaly is necessary to prevent recurrent brain abscess in cyanotic CHD.
Case analysis
The primary source of infection in this case is vegetative lesion in the heart, which in turn leads to hematogenous dissemination to brain, resulting in abscess formation, when the filtering effect of lungs, the current theory of mechanism, is circumvented in Tetralogy of Fallot and the abscess is usually solitary in children. The boy was afebrile since the fever is characteristic of early invasive phase of cerebritis and may return to normal similarly with leukocytosis when the abscess become encapsulated. The size of an abscess may not change for > 2 weeks after the institution of successful medical therapy [101] and it may took 10 weeks before the abscess resolved on CT scanning. The ineffectiveness of antibiotics in the stage of capsule formation is due to the acidic medium within the abscess cavity and the inability to have adequate therapeutic concentration of antibiotics within the abscess. Therefore, surgical treatment is essential once the capsule is well formed [102]. Stereotactic aspiration is appropriate for abscesses located in the eloquent regions of the brain because it provides a direct and rapid access to the abscess through a predetermined route. Penetration of a thick abscess wall with a blunt-tipped stereotactic probe can be difficult and so free hand aspiration technique was preferred in this case.
Outcome
Long term outcome in children included complete recovery (30 %), hemiparesis (37 %) and seizure disorder (16 %) [103]. According to four recent studies, the mortality rate of brain abscess was 13 % ( 6-24 %) [104], which had decreased substantially after the introduction of CT scanning.
Brain abscess associated with cyanotic CHD, when presented with rapidly progressive neurological deficit due to mass effect are strict candidates for urgent decompression. The resolution of surrounding edema and enhancing rim may take up to 6 months and the abnormal enhancement on CT may persists for years after the successful treatment of abscess due to mild breakdown of blood-brain barrier, but not due to residual infection [105],[106].
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation. “The peer review process was efficient and constructive, and the editorial office provided excellent communication and support throughout. The journal ensures scientific rigor and high editorial standards, while also offering a smooth and timely publication process. We sincerely appreciate the work of the editorial team in facilitating the dissemination of innovative approaches such as the Bonori Method.” Best regards, Dr. Matteo Bonori.
