
Research Article | DOI: https://doi.org/10.31579/2578-8949/074
Resident Dermatology (final year Postgraduate)
Senior professor and head, Department of dermatology, MDM hospital, Jodhpur, India
Senior professor and head, Department of dermatology, MDM hospital, Jodhpur, India
*Corresponding Author: Dilip kachhawa, senior professor and head, MDM bungalow no 3, Outside gate 3, MDM campus, Shastri Nagar, Jodhpur, India.
Citation: H Narasimhan, Pankaj Rao, D Kachhawa. (2021) Selection of anti-depressants in geriatric dermatoses- A questionnaire study of dermatologists in Western Rajasthan, India. Journal of Dermatology and Dermatitis. 6(1); Doi:10.31579/2578-8949/074
Copyright: © Dilip Kachhawa, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 May 2021 | Accepted: 14 May 2021 | Published: 17 May 2021
Keywords: geriatric dermatoses; antidepressants; polypharmacy; risk-benefit analysis
Background:
The Global Wealth Migration Review 2019 report, published by New World Wealth, estimated that 48% of India's total wealth was held by high-net worth individuals.
Distinct factors dominate the prescription of anti-depressants in the geriatric population. Accordingly, the intention of pharmacotherapy in geriatric psycho dermatoses is deciphered in the study. .
Objective: To survey and analyze the selection of anti-depressants by the dermatologists in the practice of geriatric pharmacotherapy.
Methods:
A questionnaire was designed and circulated among ninety-three dermatologists in three sessions and the data collected was analyzed through the cross-sectional study statistics.
Results:
The typical senior people attending the specialist were 25-50%. A sizeable familiarity of psycho cutaneous disturbance was attributed to dermatophyte infections, lichen simplex chronic, and Prurigo in descending order. The largely established primary disorder was neurotic excoriation. The prescription pattern was classified and 51.9% dermatologists are customary with psychotropic agent Doxepin over other agents. The discipline of the multidisciplinary approach was also studied.
Limitation: Small sample size, uniregional study, prevalence study.
Conclusions: The survey aids in evaluating mental health in cutaneous dermatoses of the elderly and assists the dermatologists to offer understated economical options and amend existing guidelines.
* Geriatric dermatoses are a mystery to the attending specialists who were surveyed to decipher the prescription of choice for individual dermatoses in daily practice in western Rajasthan, India.
* Understanding the geriatric dermatoses and newer management strategies is crucial to avoid unstructured polypharmacy and emphasizes risk: benefit analysis as needed.
* The data assists in the conformation of the existing approaches, thus refining the principles of geriatric pharmacotherapy in the skin.
Psycho-cutaneous biology is the region of dermatology that entails the intricate interactions between the skin, brain, immune system, and cutanous nerves [1]. This has expanded the responsibility of the attending specialist in sustaining the reliance of the clients. For example, a patient who cannot halt the itch-scratch cycle might lose confidence in his dermatologist, who did not foresee the coexisting psychological commotion of persistent disease.
Therefore, an expert poll was attempted in the locality of Western Rajasthan to comprehend the preference pattern of anti-psychiatric drugs in the common skin disorders of elderly The results retrieved will be extrapolated to understand the current structure of therapy.
* To understand the psychopharmacology for dermatoses of the elderly.
* To survey the preferences and alternatives of anti-psychiatric drugs by practicing Dermatologists
* To analyze the intention behind the chosen drug and to correlate with the existing policies.
The study began after ethical authorization to devise a questionnaire on anti-psychiatric agents needed in psycho-cutaneous disorders based on the existing literature. The questionnaire comprised 16 queries including the geriatric population, disease, chronicity, and preferred agent, the rationale for the options, unfavorable effects, and cure. The study group included ninety-three dermatologists working in various government colleges, private practitioners, final-year residents, and senior residents from all hospitals in Western Rajasthan. Various means were used to approach the doctors all of which were manual in a hard copy format. An appropriate elaboration was delivered before the study and written consent was obtained before participation. The study was conducted between August and September 2019.The data was collected and compiled for analysis. The results are as follows.
The all-around respondents were 90.3% (n=84), of which 3.5% did not practice psycho-pharmacotherapy.
The standard day-to-day geriatric outpatient attendance was documented to be around 25-50%. Thirty-seven percent of dermatologists claim that maximum clients used to complain about a secondary psychiatric illness and 23.5% specialists met patients with mutually dependent psychiatric and dermatologic illnesses.
The frequency prevalence of the common psycho-physiologic dermatomes experienced every day is illustrated in Figure 1, with descending frequency from dermatophyte infections (45.7% ;n=37), Lichen simplex chronicus (22.2%; n=18), Prurigo nodularis (18.5%; n=15), Urticaria (11.1%; n=9) and Psoriasis (4.9%; n=4).The primary psychiatric disorder dealt in descending commonness were neurotic excoriation (76.5%, n=62), fictitious dermatitis (14.8%; n=12), Delusional parasitosis (7.4%; n=6) and Trichitillomania (1.3%). They alleged secondary psychiatric diseases to originate from Obesity (28.4%; n=23), Androgenetic alopecia (27.2%; n=22), Acne scars (18.5%; n=15), Vitiligo (17.3%; n=14), Alopecia areata (4.9%; n=4), Keloids (2.5%; n=2) and post-burn scars (1.2%; n=1). Last, the sensory disorders acknowledged were Itching (100%; n=81), burning (63%; n=51) and both (37%; n=30).


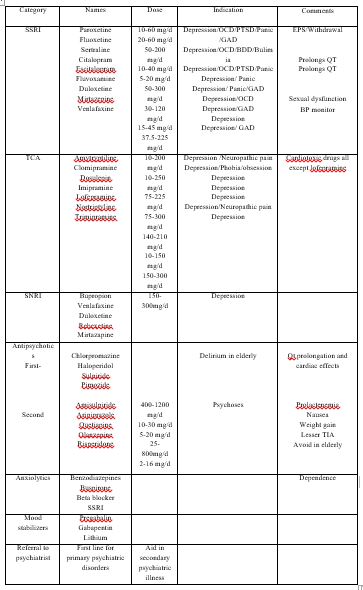
Familiar tricyclic antidepressant among study group was Doxepin (51.9%; n=42), nominated for Psychogenic prorates (85.2%; n=69) than depression (14.8%; n=12). Aftermaths are depicted in Table 3 with sedation (85.2%) and abdominal complaints (14.8%). The non-psychotropic antidepressant was inferred as being Amitriptyline (50.6%; n=41) and indicated for secondary depression (46.9%; n=38) and their adverse effects are tabulated in table 3.
Commonest SSRI was fluoxetine (56.8%; n=46) > paroxetine (28.4%; n=23) used in secondary depression (60.5%; n=49). We divulge the conclusions on Figure 1 and 2.
Multi-disciplinary attitude: Dermatologists who preferred to suggest the client to a psychiatrist at the initial visit were 86.4% (n=70).

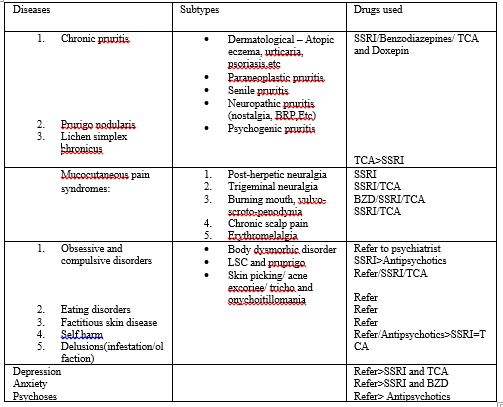
The proficiency of fundamental psycho-cutaneous disorders is decisive in practice. We can categorize these as,
1. Psycho-physiologic skin diseases like psoriasis, LSC, Hyperhidrosis that contributes to stigma and stress
2. Primary psychiatric disorders like Neurotic excoriations, delusions, fictitious dermatitis, Trichotillomania, etc.
3. Secondary psychiatric disorders like vitiligo, alopecia areata, obesity, androgenetic alopecia which are induced because of stress
4. Cutaneous sensory disorders like burning and crawling.
Psychopathology conditions- anxiety, depression, Obsession & compulsive disorder, Psychoses should be primarily managed by a psychiatrist and might often exclusively need dermatological assistance [4]
Standard regimens and their known adverse reactions are provided in Table 1. It illustrates the therapeutic ladders for specific conditions in Table 2 [3 4].
Geriatric dermatoses are the dermatoses of the aged (> or equal to 60 years of age). Yosipovitch et al., discriminated neuropathic itch from psychogenic itch which is defined as “an itching disorder where the itch is at the center of the symptomatology and where psychological factors show an obvious role in the provoking or persistence of the pruritus” [7, 11] from the survey, the structure of popular geriatric dermatoses and the established agents used by dermatologists of the locality of Western Rajasthan are analyzed and we decipher the outcomes. The customary size of the geriatric population witnessed existed from 25% to 50% which compels a promising awareness on the management of the elderly. Over 60.5% of old people attending the skin clinic might require an appropriate exam of mental health as described by Capoore and workers [1].
Commonest psycho-physiologic diseases of this era were Dermatophyte infections identified before Lichen simplex chronicus, Prurigo, Urticaria, and psoriasis. Patrol and panda deduced that dermatophyte infections move beyond its territory as investigators anticipate fungal infections as a menace to the psychological fitness of the patients [9]. Tinea is one of the most common infections experienced in our dermatological practice. Wine et al., in his study, remarks the necessity to appreciate the pattern of disease for realistic reasons [3]. For instance, the continual despair of everyday life in developing countries might be causal in impeding the recovery in an elderly man with tinea cruris, who labor in sweltering environments.
Park et al., ascribed a tool of analyses on geriatric depression and these patients should be referred to a psychiatrist after receiving the history, evaluating the co-morbidities, and gauging the emotional state based on subjective judgments [8]. Patient displaying insignificant, subsyndromal or atypical traits are extensively under-diagnosed in preliminary visits [10]. Hence, a satisfying “itch remedy” can mean a deep sense in practice. Now that a wholesome business has sprouted from the existing deadlock to determine the standard agent, the management with several over-the-counter products has led to abominable effects which is an emerging catastrophe.
The quest is to learn the idealistic parameters for an agent that is safe and psychotropic, but there is none. The patient’s dependability on the drugs is greater than the doctor’s. Thus, the agent should ease itch or provide faster clearance rates. Thus for empirical reasons, dermatologists imply in amending the textbook management for Dermatophyte using agents such as Doxepin as it is claimed to curtail the monetary and systemic burden of anti-fungal agents besides ameliorating the symptoms [1]
Some disorders are causal to the clients’ altered psyche such as Psoriasis and some are triggered e.g., Lichen simplex and Prurigo, which are familiar as age advances. Adding an SSRI (35.8%) or Doxepin (51.9%) is offered as a competent accessory [3]. the largely seen primary psycho-cutaneous disorders were neurotic excoriations (76.5% answers). The survey of antidepressants desirable to this section was SSRI (39.5%) and TCA (49.4%) but primary psychiatric illness should be referred to a psychiatrist who can benefit the patient. A pointer here is to treat the skin and refer. TCA like Amitriptyline was selected despite their speculative hazard of cardiotoxicity, reasoning that these agents are safe in practice and the probability for such consequences is diminutive (32.1% answers). Hence it is relatively a risk: benefit setting according to the pharmacological practice by Lee and his workers [5]. While the comparable safety of Fluoxetine is better than TCA, fluoxetine 20mg is determined all-around as an ideal agent (35.8%) only second to Doxepin [6].
Cases of fictitious dermatitis and Trichitillomania should also be suitably referred to Psychiatrist (86.4%). Stress donates to common secondary psycho-dermatoses like Obesity, Androgenetic alopecia, and Alopecia areata. The psychopharmacologic therapy documented by Gupta et al., indicates that adding an SSRI is not a profitable option for obesity as weight gain is overseen. Thus, suggesting to a psychiatrist who might start them on drugs like Bupropion sounds appropriate [6]. Adding a BZD or SSRI is an intriguing alternative for the rest of the illnesses [5, 7] The common antidepressants used as a psychotropic agent was Doxepin, while Benzodiazepine in Urticaria, Prurigo, and lichen simplex chronicus, SSRI in Psychogenic itch, and Amitriptyline in neuropathic itch were preferred. This also corresponds to literature.
Psychogenic itch is diagnosed after eliminating other factors of itching. For this, Co-morbidities and systemic causes should be evaluated after history and exam as discussed by Tactic and his colleagues [10]. This is crucial because diseases such as cutaneous T cell lymphoma in its premalignant stage can drive refractory prorates hence require an ethical evaluation. It was observed that Dermatologists (86.4%) are inclined to multidisciplinary referrals as and when necessary or sometimes mandatory i.e., while starting the drug while tapering and while withdrawal.
Small sample size, Uni-regional census, and prevalence study. This has to be expanded nationwide and transnational for farther awareness of prescription used around the globe. The study was a cross-sectional survey of current trends. This can be further experimented by providing a pre and postscholastic questionnaire to improve the prevailing trends and discern the readiness and aptitude of dermatologists.
The information on the structure of geriatric dermatoses and the selection of antidepressants/ psychotropic agents preferred by dermatologists is intensified in this study. There is no systematic review on this subject which broadens prospectively. This analysis also enhances the subsisting information in the practice of safer psychotropic agents and antidepressants. It comprehends the proper rationale for usage and insists on the importance of history taking, exam, investigation, and asking for help as the four cornerstones of Hippocratic practice. Similarly, psychiatrists’ hand in dealing with geriatric dermatoses is mandatory while following up and during withdrawal.
1. The primary outcome of the study is restricted to the patterns of disease and the preferred line of management
2. The secondary outcome measures were to find out the rationale behind the choice of agent. E.g., Doxepin had overall been mostly used along with SSRI (fluoxetine) and Amitriptyline hence are idealistic additional agents in prescription.
BDD- body dysmorphic disorder
BZD- benzodiazepines
EPS- extrapyramidal symptoms
GAD- generalized anxiety disorder
OCD – obsessive-compulsive disorder
PTSD- post-traumatic stress disorder
QT – wave in ECG
SSRI- selective serotonin reuptake inhibitors
TIA transient ischemic attack
TCA- tricyclic antidepressants
It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,

Dear Maria Emerson, Editorial Coordinator of International Journal of Clinical Case Reports and Reviews, What distinguishes International Journal of Clinical Case Report and Review is not only the scientific rigor of its publications, but the intellectual climate in which research is evaluated. The submission process is refreshingly free of unnecessary formal barriers and bureaucratic rituals that often complicate academic publishing without adding real value. The peer-review system is demanding yet constructive, guided by genuine scientific dialogue rather than hierarchical or authoritarian attitudes. Reviewers act as collaborators in improving the manuscript, not as gatekeepers imposing arbitrary standards. This journal offers a rare balance: high methodological standards combined with a respectful, transparent, and supportive editorial approach. In an era where publishing can feel more burdensome than research itself, this platform restores the original purpose of peer review — to refine ideas, not to obstruct them Prof. Perlat Kapisyzi, FCCP PULMONOLOGIST AND THORACIC IMAGING.
