AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/ 10.31579/2639-4162/037
1 North Manchester General Hospital Department of Urology Manchester United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital Department of Urology Manchester United Kingdom.
Citation: Anthony K-G Venyo. (2020) Schistosomiasis Associated Glomerulopathy (Glomerulonephristis / Nephrotic Syndrome): A review and Update of the Literature. General medicine and Clinical Practice. 3(4) DOI: 10.31579/2639-4162/037
Copyright: © 2020 Anthony Kodzo-Grey Venyo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 September 2020 | Accepted: 10 December 2020 | Published: 14 December 2020
Keywords: schistosomiasis, haematobium; mansoni; japonicum; mekongi; intercalatum; nephrotic syndrome; glomerulonephritis; dialysis; prevention
Schistosomiasis may affect a number of organs within the human body. Schistosomiasis may also be associated with glomerular disease of the kidney in the form of glomerulonephritis and nephrotic syndrome. The association between Schistosomiasis and glomerulopathy may not be well known by a number of practitioners and its pathophysiology may not be very well understood and this could be due to the underdiagnosis of the disease due to the possibility of lack of facilities within the Schistosomiasis endemic areas of the world especially within tropical Africa. Nevertheless, there are a number of patterns of renal involvement in Schistosomiasis which include (a) upper urinary tract sequelae of lower urinary tract Schistosomiasis pathology, (b) immune-related glomerulonephritis, (c) as well as oxidant-stress-mediated renal tubular glomerulonephritis. The renal involvement by Schistosomiasis does tend to be ensued by the development of Schistosomiasis-associated Glomerulopathy (Glomerulonephritis / Nephrotic Syndrome) of varying severity. Individuals affected by Schistosomiasis-associated kidney disease may develop (a) asymptomatic disease which tends to related to self-limited and asymptomatic glomerular disease (b) symptomatic disease which most commonly would tend to present with nephrotic syndrome most often in patients who develop hepato-splenic schistosomiasis with liver fibrosis associated with Schistosoma mansoni infection. Symptomatic patients tend to develop severe hypo-proteinemia, half of the patients tend to have elevated blood pressure. In the absence of nephrotic syndrome, patients who have Schistosomiasis-associated glomerulopathy may manifest with: (a) isolated non-nephrotic syndrome proteinuria (b) acute glomerulonephritis associated with haematuria and heavy proteinuria, (c) Nephrotic syndrome together with systemic manifestations of co-infection with salmonella (class II) or hepatitis C virus (Class I), (d) End stage renal disease (ESRD). Some of the patients who have Schistosomiasis of the kidney may present with Haematuria, Hypertension, Hepato-splenic Schistosomiasis. The diagnosis should be suspected with regard to the following scenarios: (a) clinical suspicion in a patient with kidney disease who is known or has been known to have Schistosoma mansoni; (b) exposure to an endemic area, (c) clinical evidence / demonstration of chronic hepatosplenic schistosomiasis, (d) if the patient has not been diagnosed as having been afflicted with schistosomiasis, then schistosomal infection should be documented, (e) majority of patients with schistosomiasis and kidney disease should have kidney biopsy. (f) The patients should be evaluated for co-infection with salmonella, hepatitis C virus, and hepatitis B virus in order to ensure adequate treatment of the disease. Schistosomiasis is the second most devastating tropical parasitic disease globally which tends to be responsible for many urological complications. Nevertheless, glomerular injury is an uncommon complication which has mainly or most often described with Schistosoma Mansoni. When patients who have Schistosomiasis-associated Kidney disease are managed and followed-up on long-term basis with renal end points, one third of the patients independent of the histopathology examination features of the kidney biopsies would tend to progress dialysis. Membranoproliferative glomerulonephritis (MPGN) is an uncommon complication associated with Schistosoma Haematobium infection which tends to be associated with potentially poor prognosis. MPGN could lead quickly to End Stage Renal Disease (ESRD). Anti-helminthic and immunosuppressive medicaments tend not to be effective at advanced stages of the disease and hence efforts need to be focused upon the prevention, early detection, as well as treatment of Schistosoma infections among at-risk groups of individuals. In order to reduce morbidity related to Schistosoma-associated nephropathy, public health policy, should be concentrated upon the prevention of the disease by the control of snail, improved sanitation, and health education, as well as by the implementation, and sustenance of chemotherapy-based control strategies. Considering that many individuals are found yearly to be inflicted by Schistosomiasis who tend to dwell in more rural parts of their countries where facilities for the undertaking of renal function tests and biopsies of the kidney tend not to be readily available, there is the likelihood that Schistosomiasis-associated nephropathies may be highly underdiagnosed globally.
Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Pathophysiology
Acute Schistosomiasis (Katayama syndrome)
Katayama syndrome which is an acute schistosomiasis is a terminology which describes a systemic serum sickness-like ailment which develops after a number of weeks in some patients but this does not occur in most patients with new schistosoma infections. Ahmed et al. [5] stated that:
Chronic schistosomiasis
Ahmed et al. [5] stated that chronic schistosomiasis is more common in comparison with acute schistosomiasis. They also stated that:
Aetiology
The Center for Disease Control and Prevention has made the ensuing summations related to the causative agents of Schistosomiasis as follows: [19]
Schistosomiasis (Bilharziasis) is stated to be caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species that tend to infect human beings include Schistosoma haematobium, Schistosoma Japonicum, and Schistosoma Mansoni. Three other species of Schistosoma exist which tend to be more localized geographically, which include Schistosoma Mekongi, Schistosoma Intercalatum, as Shistosoma Guineensis that was previously considered to be synonymous with Schistosoma intercalatum. It has been iterated that there had also been a few reported cases of hybrid Schistosomes of cattle origin (Schistosoma haematobium, x Schistosoma bovis, X Schistosoma curassani, x Schistosoma mattheei which had infected human beings. Unlike trematodes, which are hermaphroditic, Schistosoma spp. are said to be dioicous (individuals of separate sexes). It has been furthermore, iterated that other species of Schistosomes exist, which tend to parasitize birds as well as mammals, and they could cause cercarial dermatitis within human beings but this is clinically distinct from Schistosomiasis.

Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Pathophysiology
Acute Schistosomiasis (Katayama syndrome)
Katayama syndrome which is an acute schistosomiasis is a terminology which describes a systemic serum sickness-like ailment which develops after a number of weeks in some patients but this does not occur in most patients with new schistosoma infections. Ahmed et al. [5] stated that:
Chronic schistosomiasis
Ahmed et al. [5] stated that chronic schistosomiasis is more common in comparison with acute schistosomiasis. They also stated that:
Aetiology
The Center for Disease Control and Prevention has made the ensuing summations related to the causative agents of Schistosomiasis as follows: [19]
Schistosomiasis (Bilharziasis) is stated to be caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species that tend to infect human beings include Schistosoma haematobium, Schistosoma Japonicum, and Schistosoma Mansoni. Three other species of Schistosoma exist which tend to be more localized geographically, which include Schistosoma Mekongi, Schistosoma Intercalatum, as Shistosoma Guineensis that was previously considered to be synonymous with Schistosoma intercalatum. It has been iterated that there had also been a few reported cases of hybrid Schistosomes of cattle origin (Schistosoma haematobium, x Schistosoma bovis, X Schistosoma curassani, x Schistosoma mattheei which had infected human beings. Unlike trematodes, which are hermaphroditic, Schistosoma spp. are said to be dioicous (individuals of separate sexes). It has been furthermore, iterated that other species of Schistosomes exist, which tend to parasitize birds as well as mammals, and they could cause cercarial dermatitis within human beings but this is clinically distinct from Schistosomiasis.
Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Pathophysiology
Acute Schistosomiasis (Katayama syndrome)
Katayama syndrome which is an acute schistosomiasis is a terminology which describes a systemic serum sickness-like ailment which develops after a number of weeks in some patients but this does not occur in most patients with new schistosoma infections. Ahmed et al. [5] stated that:
Chronic schistosomiasis
Ahmed et al. [5] stated that chronic schistosomiasis is more common in comparison with acute schistosomiasis. They also stated that:
Aetiology
The Center for Disease Control and Prevention has made the ensuing summations related to the causative agents of Schistosomiasis as follows: [19]
Schistosomiasis (Bilharziasis) is stated to be caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species that tend to infect human beings include Schistosoma haematobium, Schistosoma Japonicum, and Schistosoma Mansoni. Three other species of Schistosoma exist which tend to be more localized geographically, which include Schistosoma Mekongi, Schistosoma Intercalatum, as Shistosoma Guineensis that was previously considered to be synonymous with Schistosoma intercalatum. It has been iterated that there had also been a few reported cases of hybrid Schistosomes of cattle origin (Schistosoma haematobium, x Schistosoma bovis, X Schistosoma curassani, x Schistosoma mattheei which had infected human beings. Unlike trematodes, which are hermaphroditic, Schistosoma spp. are said to be dioicous (individuals of separate sexes). It has been furthermore, iterated that other species of Schistosomes exist, which tend to parasitize birds as well as mammals, and they could cause cercarial dermatitis within human beings but this is clinically distinct from Schistosomiasis.
Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Pathophysiology
Acute Schistosomiasis (Katayama syndrome)
Katayama syndrome which is an acute schistosomiasis is a terminology which describes a systemic serum sickness-like ailment which develops after a number of weeks in some patients but this does not occur in most patients with new schistosoma infections. Ahmed et al. [5] stated that:
Chronic schistosomiasis
Ahmed et al. [5] stated that chronic schistosomiasis is more common in comparison with acute schistosomiasis. They also stated that:
Aetiology
The Center for Disease Control and Prevention has made the ensuing summations related to the causative agents of Schistosomiasis as follows: [19]
Schistosomiasis (Bilharziasis) is stated to be caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species that tend to infect human beings include Schistosoma haematobium, Schistosoma Japonicum, and Schistosoma Mansoni. Three other species of Schistosoma exist which tend to be more localized geographically, which include Schistosoma Mekongi, Schistosoma Intercalatum, as Shistosoma Guineensis that was previously considered to be synonymous with Schistosoma intercalatum. It has been iterated that there had also been a few reported cases of hybrid Schistosomes of cattle origin (Schistosoma haematobium, x Schistosoma bovis, X Schistosoma curassani, x Schistosoma mattheei which had infected human beings. Unlike trematodes, which are hermaphroditic, Schistosoma spp. are said to be dioicous (individuals of separate sexes). It has been furthermore, iterated that other species of Schistosomes exist, which tend to parasitize birds as well as mammals, and they could cause cercarial dermatitis within human beings but this is clinically distinct from Schistosomiasis.
Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Pathophysiology
Acute Schistosomiasis (Katayama syndrome)
Katayama syndrome which is an acute schistosomiasis is a terminology which describes a systemic serum sickness-like ailment which develops after a number of weeks in some patients but this does not occur in most patients with new schistosoma infections. Ahmed et al. [5] stated that:
Chronic schistosomiasis
Ahmed et al. [5] stated that chronic schistosomiasis is more common in comparison with acute schistosomiasis. They also stated that:
Aetiology
The Center for Disease Control and Prevention has made the ensuing summations related to the causative agents of Schistosomiasis as follows: [19]
Schistosomiasis (Bilharziasis) is stated to be caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species that tend to infect human beings include Schistosoma haematobium, Schistosoma Japonicum, and Schistosoma Mansoni. Three other species of Schistosoma exist which tend to be more localized geographically, which include Schistosoma Mekongi, Schistosoma Intercalatum, as Shistosoma Guineensis that was previously considered to be synonymous with Schistosoma intercalatum. It has been iterated that there had also been a few reported cases of hybrid Schistosomes of cattle origin (Schistosoma haematobium, x Schistosoma bovis, X Schistosoma curassani, x Schistosoma mattheei which had infected human beings. Unlike trematodes, which are hermaphroditic, Schistosoma spp. are said to be dioicous (individuals of separate sexes). It has been furthermore, iterated that other species of Schistosomes exist, which tend to parasitize birds as well as mammals, and they could cause cercarial dermatitis within human beings but this is clinically distinct from Schistosomiasis.
Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Pathophysiology
Acute Schistosomiasis (Katayama syndrome)
Katayama syndrome which is an acute schistosomiasis is a terminology which describes a systemic serum sickness-like ailment which develops after a number of weeks in some patients but this does not occur in most patients with new schistosoma infections. Ahmed et al. [5] stated that:
Chronic schistosomiasis
Ahmed et al. [5] stated that chronic schistosomiasis is more common in comparison with acute schistosomiasis. They also stated that:
Aetiology
The Center for Disease Control and Prevention has made the ensuing summations related to the causative agents of Schistosomiasis as follows: [19]
Schistosomiasis (Bilharziasis) is stated to be caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species that tend to infect human beings include Schistosoma haematobium, Schistosoma Japonicum, and Schistosoma Mansoni. Three other species of Schistosoma exist which tend to be more localized geographically, which include Schistosoma Mekongi, Schistosoma Intercalatum, as Shistosoma Guineensis that was previously considered to be synonymous with Schistosoma intercalatum. It has been iterated that there had also been a few reported cases of hybrid Schistosomes of cattle origin (Schistosoma haematobium, x Schistosoma bovis, X Schistosoma curassani, x Schistosoma mattheei which had infected human beings. Unlike trematodes, which are hermaphroditic, Schistosoma spp. are said to be dioicous (individuals of separate sexes). It has been furthermore, iterated that other species of Schistosomes exist, which tend to parasitize birds as well as mammals, and they could cause cercarial dermatitis within human beings but this is clinically distinct from Schistosomiasis.
Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Pathophysiology
Acute Schistosomiasis (Katayama syndrome)
Katayama syndrome which is an acute schistosomiasis is a terminology which describes a systemic serum sickness-like ailment which develops after a number of weeks in some patients but this does not occur in most patients with new schistosoma infections. Ahmed et al. [5] stated that:
Chronic schistosomiasis
Ahmed et al. [5] stated that chronic schistosomiasis is more common in comparison with acute schistosomiasis. They also stated that:
Aetiology
The Center for Disease Control and Prevention has made the ensuing summations related to the causative agents of Schistosomiasis as follows: [19]
Schistosomiasis (Bilharziasis) is stated to be caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species that tend to infect human beings include Schistosoma haematobium, Schistosoma Japonicum, and Schistosoma Mansoni. Three other species of Schistosoma exist which tend to be more localized geographically, which include Schistosoma Mekongi, Schistosoma Intercalatum, as Shistosoma Guineensis that was previously considered to be synonymous with Schistosoma intercalatum. It has been iterated that there had also been a few reported cases of hybrid Schistosomes of cattle origin (Schistosoma haematobium, x Schistosoma bovis, X Schistosoma curassani, x Schistosoma mattheei which had infected human beings. Unlike trematodes, which are hermaphroditic, Schistosoma spp. are said to be dioicous (individuals of separate sexes). It has been furthermore, iterated that other species of Schistosomes exist, which tend to parasitize birds as well as mammals, and they could cause cercarial dermatitis within human beings but this is clinically distinct from Schistosomiasis.
Schistosomiasis (Bilharziasis) is caused by tremades (blood flukes) of the genius Schistisoma. The WHO fact sheet No 115, [1] has ranked Schistosomiasis as the third most tropical disease globally after malaria and intestinal worms (helminthiasis). The Who fact sheet No 115, [1] also indicated that Schistosomiasis is a major cause of morbidity and mortality in developing countries in Africa, South America, the Caribbean, the Middle East and Asia. [1]Documentation from World Health Organization data [1] indicated that more than 207 million people globally have been afflicted with Schistosomiasis and 85% of the afflicted patients reside in Africa. World Health Organization documentations [1] [2] also estimated that in 76 countries where Schistosomiasis had been regarded as an endemic disease 700 million individuals face the risk for the development of the disease. These documentations additionally indicated that agricultural work, domestic chores and recreational activities had exposed individuals who had developed schistosomiasis to infested water. [1] [2] Chistulo et al. [3] stated that world-wide, 200,000 deaths had been attributed to schistosomiasis yearly. It had been intimated that Schistosomiasis, which is also called bilharziasis, or snail fever, was discovered by Theodore Bilharz, a German Surgeon who had worked in Cairo and that in 1851 Theodore Bilharz identified Schistosoma haematobium as the cause of the disease. [4]] It has been stated that most cases of Schistosomiasis affecting human beings are caused by Schistosoma haematobium, Schistosoma mansoni, and Schistosoma Japonicum; nevertheless, other less common species, including Schistosoma mekongi and Schistosoma intercalatum may also be responsible for systematic human disease of Schistosomiasis. [5] Furthermore, it has been iterated that other types of Schistosoma organisms with avian or mammalian primary hosts may result in the development of severe dermatitis by human beings for example, swimmers itch which ensues Trichobilharzia coellata. Most clinicians would be aware of the fact that Schistosomiasis haematobium tends to present with haematuria and that carcinoma of the urinary bladder tends to manifest many years after the patient had had initial symptoms related to Schistosomiasis. Generally clinicians would be aware of the common causes of glomerulonephritis and nephrotic syndrome. In view of the fact schistosomiasis is not on the top list of causes of nephropathy a number clinicians could easily overlook the possibility of schistosomiasis being associated with nephropathy. The ensuing literature review on schistosomiasis is divided into two parts: (A) An overview which has summarized various aspects of Schistosomiasis in general; and (B) which contains miscellaneous narrations and discussions from a number of reported cases, case series and reviews related to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome)
Method
Internet data bases were searched including: Google; Google scholar, Yahoo, Bing, Research gate, and PUBMED. The search words that were used included: Schistosomiasis; Schistosoma Haematobium; Schistosoma Mansoni; Schistosoma Japonicum; Schistosoma Intercalatum; Schistosoma Mekongi, Schistosoma glomerulopathy; Schistosoma nephropathy; Schistosoma glomerulonephritis; Schistosoma nephrotic syndrome; Bilharziasis nephropathy; Bilharziasis glomerulonephritis; Bilharzia nephrotic syndrome; Schistosoma-associated nephropathy. Ninety two references were identified which were used to write the review and update of the literature on Schistosomiasis-associated nephropathy which has been divided into two parts: (A) Overview of Schistosomiasis in general and Schistosomiasis nephropathy and (B) Miscellaneous narrations from some case reports, case series and studies related to Schistosomiasis-associated nephropathy/nephrotic syndrome.
Review and Update of Literature.
General characteristics of Schistosomiasis
The pathological process that is associated with Schistosomiasis (Bilharziasis) is related to the immunohistological reactions of the patient to Schistosoma eggs which have been trapped in the tissues of the patient. [5] It has been stated that:
A number of authors [6] [7] [8] had iterated that:
Snail hosts
Different types of snails serve as the intermediate hosts for the various types of Schistosomiasis causing organisms as follows which tend to divided into urogenital Schistosomiasis and intestinal Schistosomiasis causing snail hosts:
Urogenital Schistosomiasis
Intestinal Schistosomiasis
Complications
Various complications and presentations may be encountered in patients with Schistosomiasis depending upon the type of schistosomiasis and the organ involved. Some of the findings and complications include [5]:
Pathophysiology
Acute Schistosomiasis (Katayama syndrome)
Katayama syndrome which is an acute schistosomiasis is a terminology which describes a systemic serum sickness-like ailment which develops after a number of weeks in some patients but this does not occur in most patients with new schistosoma infections. Ahmed et al. [5] stated that:
Chronic schistosomiasis
Ahmed et al. [5] stated that chronic schistosomiasis is more common in comparison with acute schistosomiasis. They also stated that:
Aetiology
The Center for Disease Control and Prevention has made the ensuing summations related to the causative agents of Schistosomiasis as follows: [19]
Schistosomiasis (Bilharziasis) is stated to be caused by some species of blood trematodes (flukes) in the genus Schistosoma. The three main species that tend to infect human beings include Schistosoma haematobium, Schistosoma Japonicum, and Schistosoma Mansoni. Three other species of Schistosoma exist which tend to be more localized geographically, which include Schistosoma Mekongi, Schistosoma Intercalatum, as Shistosoma Guineensis that was previously considered to be synonymous with Schistosoma intercalatum. It has been iterated that there had also been a few reported cases of hybrid Schistosomes of cattle origin (Schistosoma haematobium, x Schistosoma bovis, X Schistosoma curassani, x Schistosoma mattheei which had infected human beings. Unlike trematodes, which are hermaphroditic, Schistosoma spp. are said to be dioicous (individuals of separate sexes). It has been furthermore, iterated that other species of Schistosomes exist, which tend to parasitize birds as well as mammals, and they could cause cercarial dermatitis within human beings but this is clinically distinct from Schistosomiasis.
Schistosoma eggs are eliminated with faeces or urine, depending on species

. Under appropriate conditions the eggs hatch and release miracidia

, which swim and penetrate specific snail intermediate hosts

. The stages in the snail include two generations of sporocysts

and the production of cercariae

. Upon release from the snail, the infective cercariae swim, penetrate the skin of the human host

, and shed their forked tails, becoming schistosomulae

. The schistosomulae migrate via venous circulation to lungs, then to the heart, and then develop in the liver, exiting the liver via the portal vein system when mature,


. Male and female adult worms copulate and reside in the mesenteric venules, the location of which varies by species (with some exceptions)

. For instance, S. japonicum is more frequently found in the superior mesenteric veins draining the small intestine

, and S. mansoni occurs more often in the inferior mesenteric veins draining the large intestine

. However, both species can occupy either location and are capable of moving between sites. S. intercalatum and S. guineensis also inhabit the inferior mesenteric plexus but lower in the bowel than S. mansoni. S. haematobium most often inhabitsin the vesicular and pelvic venous plexus of the bladder

, but it can also be found in the rectal venules. The females (size ranges from 7–28 mm, depending on species) deposit eggs in the small venules of the portal and perivesical systems. The eggs are moved progressively toward the lumen of the intestine (S. mansoni,S. japonicum, S. mekongi, S. intercalatum/guineensis) and of the bladder and ureters (S. haematobium), and are eliminated with faeces or urine, respectively
.
CDC has iterated the following: [19]
Clinical Manifestation
The CDC has made summating iterations related to the manifestations of various types of Schistosomiasis as follows: [19]
Epidemiology
Estimates of Schistosomiasis Infection
In 2010, approximately 238 million people were stated to have been infected with Schistosomiasis and out of these, 85% of the patients were stated to live within Africa [23]. It had also been iterated that an earlier estimate of cases of global Schistosomiasis from 2006, had documented the number of individuals who had been infected with Schistosomiasis was 200 million. [24] It has also been iterated that within many parts of the Schistosomiasis affected areas, Schistosomiasis does infest a large proportion of children who tend to be younger than 14 years of age. It has also been iterated that an estimated 600 million to 700 million individuals globally are at risk for the development of Schistosomiasis in view of the fact that they dwell within countries in which Schistosoma organism is common. [20] It has been documented that in 2012, 249 million had needed therapy in order to prevent the development of Schistosomiasis. Also it iterated that in 2014 it was estimated that the total number of people that required treatment for Schistosomiasis was 258 875 452 of whom 123 329 536 that amounted to 47.6% of people requiring treatment for Schistosomiasis were school age children whose ages were between 5 years and 14 years. In 2014 91.4% of the people who were estimated to require treatment for Schistosomiasis were living within the continent of Africa. [25] It has additionally been documented that the aforementioned estimated figures of Schistosomiasis infections would perhaps make Schistosomiasis, the commonest global parasitic infection with malaria perhaps the second most common parasitic global infection and which tend to cause approximately 207 million cases of infection in 2013 based upon the stipulations of some authors. [20] It has furthermore, been iterated that Schistosomiasis is also referred to as snail fever as well as bilharzia [26] which is caused by schistosomes and despite the high incidence of the disease it has been listed as a neglected tropical disease. [20] It was documented in Malaria Fact Sheet No. 94 which was updated in March 2014 that in 2012, malaria caused an estimated 627 000 deaths with an uncertainty range of 473 000 to 789 000 which mostly involved African children. It was additionally documented that based upon the latest estimates that were released in December 2013, there were 207 million cases of malaria in 2012 with an uncertainty range of 135 million to 287 million as well as an estimated 627 000 deaths with an uncertainty range of 473 000 to 789 000 as well as the mortality rates of malaria had fallen by 42% globally since 2000, and by 49% within the WHO African Region. [27] It has been documented that Schistosoma Haematobium which tends to be mainly. responsible for infections of the genitourinary tract does infect more than 112 million individuals yearly within Sub-Saharan Africa alone. [20] [28] Schistosoma Haematobium has been iterated to be responsible for 32 million cases of dysuria, 10 million cases of hydronephrosis, and 150 million cases of death that emanate from kidney failure each year, which would tend to make Schistosoma Haematobium the World’s deadliest Schistosome. [20] [28] Considering the large number of cases of various types of Schistosoma infections that are encountered globally each year and the few cases of kidney biopsies that tend to be undertaken in rural parts of the world where Schistosomiasis tend to be more commonly encountered, there is the likelihood that many cases of Schistosoma infection-associated nephropathy could be missed or underdiagnosed.
Deaths related to Schistosomiasis
It has been documented that estimates related to the number of deaths related to Schistosomiasis have varied. [20] It has been iterated that globally, the Global burden of Disease Study in 2010 had estimated deaths directed related to the disease at 12,000 while the World Health Organization (WHO) in 2014, had estimated greater than 200,000 annual deaths that had been related to Schistosomiasis. [20] [29] It has also been documented that another 20 million individuals had developed severe consequences related to Schistosomiasis. It has also been stated that the estimates of death related to Schistosomiasis do need to be reassessed in view of the fact that the death rate has varied between 24,072 and 200,000 globally each year. In 2000, the World Health Organization did estimate the annual death rate of Schistosomiasis as 200,000 globally and this is expected to have decreased considerably in view of the impact of a scale-up in large chemotherapy campaigns over the preceding decade. It has been documented that the control of Schistosomiasis has been successfully implemented over the preceding 40 years in many countries with the inclusion of Brazil, Cambodia, China, Egypt, Mauritius, Islamic Republic of Iran, Oman, Jordan, Saudi Arabia, Morocco, Tunisia and other countries. It has also been documented that in Burundi, Burkina Faso, Ghana, Niger, Rwanda, Sierra Leone, the United Republic of Tanzania, and Yemen, there has been the possibility to scale-up the treatment of Schistosomiasis to the national level and this has had an impact on the disease over a few years. It has been recommended that an assessment of the status of transmission of Schistosomiasis is needed in many countries. [10] It has also been iterated that Schistosomiasis, is the deadliest of the neglected tropical diseases. [20]
History of Schistosomiasis
Race-related demographics
Ahmed et al. [5] stated that:
Sex-related demographics
It has been documented that [5]:
Age-related demographics
The age-related demographics of schistosomiasis has been summarized as follows [5]:
Treatment
Two medicaments namely praziquantel and Oxamniquine are available to be utilized for the treatment of Schistosomiasis. [37] The two medicaments have been stated to be considered as equivalent with regard to their efficacy against Schistosoma Mansoni and their safety. [37] It has additionally been iterated that in view of the fact that Praziquantel has lower cost per each treatment, and the fact that Oxaminiquine does tend not to be efficacious against the urogenital form of Schistosomiasis that is caused by Schistosoma Haematobium, generally, Praziquantel has been regarded the first option of treatment for Schistosomiasis. [38] The aim of treatment of Schistosomiasis is to ensure cure of the disease and to prevent the progression of the acute form of Schistosomiasis to the chronic form of Schistosomiasis. It has been strongly recommended that all cases of suspected Schistosomiasis should be treated irrespective of their manifestation in view of the fact that the adult parasite could live within the host for many years. [20] [39] It has been stipulated that Schistosomiasis can be treated by means of the taking orally of a single dose of Praziquantel medicament annually [20] It has been documented that the World Health Organization has developed guidelines pertaining to the community treatment based upon the impact the disease tends to have on children within villages in which the disease is common as follows: [20]
Other possible options of treatment for Schistosomiasis do include: utilization of a combination of praziquantel with metrifonate, artesunate, or mefloquine, or mefloquine. [40] It has been documented that a Cochrane review of the literature had found tentative evidence which had documented that utilization of metrifonate alone was as effective as praziquantel with regard to the treatment of Schistosomiasis. [40] Another medicament, mefloquine, which had previously been utilized with regard to the treatment of as well as prevention of malaria, had been recognized between 2008 and 2009 to be effective as treatment for Schistosomiasis. [41] It has been pointed out that historically, utilization of antimony potassium tartrate had remained the treatment option of choice with regard to the management of Schistosomiasis until praziquantel was developed in the 1980s. [42]
Acute Schistosomiasis (Katayama Syndrome)
Chronic Schistosomiasis
Gastrointestinal Schistosomiasis
Lapa et al. [11] stated that:
Schistosomiasis of the urinary tract
Ahmed et al. [5] stated that schistosomiasis of the urinary tract emanate in renal failure as a sequel of obstructive uropathy, pyelonephritis, or carcinoma of the urinary bladder which tends to occur 10 years to 20 years after the initial infection and furthermore, immune complexes which contain worm antigens may be deposited in the glomeruli which can lead to glomerulonephritis and amyloidosis.
Schistosomiasis of the Female Genital tract
Mosunjac et al. [43] iterated that Schistosoma haematobium does cause lesions in the lower genital tract of female patients including the cervix, vulva and vagina and that schistosomiasis of the female genital tract has been documented to be a major social and medical problem which may enhance the spread of some sexually transmitted diseases including HIV and human papillomavirus (HPV)
Co-existence of sexually transmitted infection and urogenital schistosomiasis
Leutscher et al. [44] reported their study in which the ensuing observations were made:
It has been stated that HIV replication and cytokine dysregulation does occur in the presence of schistosomiasis in HIV-positive individuals and that immune restoration syndrome had been described with symptomatic schistosomiasis in patients who had been taking anti-retroviral treatment. [5]
Schistosomiasis in pregnancy
Friedman et al. [45] in 2007, reported an association between schistosomiasis in pregnancy with anaemia and low birth weight.
Summary of salient points specifically related to Schistosomiasis glomerulonephritis and nephrotic syndrome
Epidemiology
Schistosomiasis glomerular disease
Barsoum [46] stated that the incidence of Schistosomiasis glomerular disease is not known in view of the fact that most cases of schistosomiasis associated glomerular disease are sub-clinical or resolve spontaneously [46]. Essat et al. [47] [48] stated that in a village in Upper Egypt, where Schistosoma haematobium was introduced because of changing irrigation methods, most of the people who acquired the infection developed self-limited nephrotic range proteinuria with biopsy confirmed mesangioproliferative glomerulonephritis. It has been stated that similar glomerular lesions had also been described with recent schistosoma mansoni or schistosoma japonicum infection and they usually resolved following antibiotic treatment. [46] Nevertheless, a number of authors, [49] [50] [51] [52] [53] had reported persistent or progressive glomerular disease in about 10% to 15% of patients who had developed hepatic fibrosis due to chronic infection with Schistosoma mansoni and also occasionally. Schistosoma haematobium
Pathogenesis
A number of observations had been made which would indicate a pathogenic role for the immune response to the Schistosoma parasite in the development of glomerulonephritis in patients affected by the disease as follows:
Sobh et al. [52] indicated that the glomerular injury which occurs in Schistosomiasis glomerulopathy is a sequel of antigens which are released by Schistosoma worms within the tributaries of the portal vein. Nevertheless, progression to advanced pathological lesions and eventual glomerulosclerosis has been postulated to be associated with a variety of factors which include:
Clinical and Pathological presentations of schistosomiasis glomerulopathy [Clinicopathological presentation [clinical manifestations; and co-infections]
The clinical manifestations were summarized by Barsoum et al. [46] as follows:
With regard to outcome, Barsoum [46] stated that majority of patients who are asymptomatic with incidentally diagnosed non-nephrotic proteinuria would recover following anti-parasitic treatment. On the other hand, majority of the symptomatic patients would develop progressive renal disease and end up developing end stage renal disease (ESRD) or they would die as a result of other complications of fibrosis of the liver.
Salmonella co-infection
With regard to Salmonella infection, the patients tend to have a rapid onset of nephrotic syndrome and an active urine sediment which show red and white cell casts [46]. Barsoum et al. [68] stated that the renal function may be impaired as a sequel of sepsis and hypovolaemia and that the serum complement C3 tends typically to be reduced as a result of alternative pathway activation by bacterial endotoxin, and the patients might additionally have positive serological tests for syphilis, rheumatoid factor, anti-nuclear antibodies, and anti-DNA antibodies. Barnhill et al. [70] indicated that the disease tends to be reversible with combined anti-parasitic and antibiotic treatment.
Histological classification
Barsoum [46] stated that: (a) The African Association of Nephrology (AFRAN) had approved the classification of schistotomal glomerulopathies into five categories based on the prevailing histopathological lesions [51] and (b) As a result of the increasing incidence of co-infection a sixth category has been proposed to increase the categories of glomerulopathies to six. The categories of glomerulopathies have been summarized as follows:
In addition to the five accepted categories and the proposed sixth category of schistosomal glomerulopathy, some authors [51] [52] [53] have pointed out that there are other patients with schistosomiasis as well as heavy proteinuria are observed to have membraneous nephropathy (MN) but this group of patients have not yet been included in the AFRAN classification as a result of the fact that so far there is lack of evidence for a pathogenic link.
Diagnosis
Barsoum [46] stated that a sequence of steps, are important in the process of the diagnosis of schstosomal glomerulopathy and that: The diagnosis commences or should be suspected: (a) with the clinical suspicion in a patient with kidney disease who is known or has been known to have schistosoma mansoni; (b) exposure to an endemic area, (c) clinical evidence / demonstration of chronic hepatosplenic schistosomiasis, (d) if the patient has not been diagnosed as having been afflicted with schistosomiasis, then schistosomal infection should be documented, (e) majority of patients with schistosomiasis and kidney disease should have kidney biopsy. (f) The patients should be evaluated for co-infection with salmonella, hepatitis C virus, and hepatitis B virus
Barsoum [46] further stated that:
Documentation of schistosoma infection
Barsoum et al. [46] intimated that:
The place of renal biopsy; and screening
Barsoum et al. [46] intimated that a biopsy of the kidney is usually indicated unless the kidney disease is benign. They stated further that:
Screening
Barsoum et al. [46] iterated that considering the fact that patients who have been afflicted with hepatosplenic schistosomiasis and fibrosis of the liver have a high risk of developing glomerulopathy, even following effective anti-parasitic treatment, they would make the ensuing suggestions:
Such patients with no known kidney disease should be screened for kidney disease yearly with the use of (a) urine dipstick testing looking for proteinuria and haematuria and (b) serum creatinine. In the event of confirmation of an abnormal urine dipstick finding after repeat testing, the urine sediment must be examined and the proteinuria should be quantified by means of urine protein-to-creatinine ratio
Differential diagnosis
Barsoum et al. [46] stated that:
Dash and Bhowmik [75] stated that:
Barsoum et al. [46] stated that even though IgA nephropathy can occur in nephrotic syndrome and ESRD, such patients do not tend to have liver fibrosis.
Treatment and outcome
Some authors [74] [76] had stated that the treatment of schistosomiasis-associated glomerular disease is pivoted around treatment of the underlying helminthic infection. Nevertheless, the clinical outcome varies according to the histological class of the disease. They also stated that immunosuppressive treatment is not warranted in patients with schistosomiasis-associated glomerular disease.
Class I disease
With regard to Class I disease, Barsoum [51] stated that the disease may remain sub-clinical, regress either spontaneously or with anti-parasitic therapy, or it may progress by transformation into other classes depending upon the presence of co-infections (for example, transformation into class II or VI), the presence of liver fibrosis (for example, transformation into class III or IV), presence of certain genetic polymorphisms
Mahmoud [77] stated that Class I Schistosomal glomerular disease, especially, in the presence of living ova in stools or rectal snip should be treated with praziquantel.
Class II disease
The treatment of class II disease has been summarized in the ensuing statements:
Class II disease is reversible with simultaneous or sequential treatment of the schistosomiasis by means of praziquantel medication and salmonella with antibiotics like ampicillin, trimethoprim-sulfamethoxazole as reported by Tsang and Wilson [74] or ciprofloxacin as reported by Bassily et al. [78]. Barnhill et al. [79] stated that treatment against salmonella alone would not be effective in view of the fact that these bacteria firmly attach to schistosomal worms and they hide under a protective layer of host proteins which covers the worms.
Other classes of disease (Class III, IV, and V)
Some authors [76] [80] stated that Class III, IV, and V disease progress relentlessly ending up in end-stage renal disease (ESRD) over a period of four to six years, irrespective of treatment. Barsoum [71] recommended that the schistosomiasis should be treated with an anti-parasitic medication, even though such treatment would unlikely lead to improvement in the renal disease and that immunotherapy drugs are not indicated for the treatment of these classes of the disease. Barsoum [71] also stated that:
Patients with class VI disease tend to go through a rapid clinical deterioration commonly, as a result of associated liver disease and severe hypoproteinemia.
A number of patients succumb to inter-current infection even prior to reaching end-stage renal disease.
It has been documented that Class VI glomerular disease is resistant to both anti-parasitic and antiviral therapy and clearance of hepatitis C viral infection improves difficult to achieve with the presence of schistosomal liver fibrosis. [81]
[B] Miscellaneous narrations and discussions from some reported cases, case series and review papers relating to Schistosomiasis associated glomerulopathy (glomerulonephritis and nephrotic syndrome
Neves et al. [82] stated that within Brazil, Schistosomiasis tends to be caused by Schistosoma Mansoni, which tend to occur within the North Eastern and South Eastern regions of the country. They additionally iterated that Schistosomiasis primarily, does affect the liver and the gastrointestinal tract, even though the kidneys could also be affected by the disease and this kidney affection by Schistosoma Mansoni has mainly been in the form of glomerulopathies. Neves et al. [82] described the characteristic features of patients who develop Schistosomiasis-associated glomerulopathies, including the management and kidney outcomes. Neves et al. [82] undertook a retrospective analysis of patients who had been diagnosed as having Schistosomiasis-associated glomerulopathy between 2002 and 2017. They evaluated the clinical, biochemical, as well as the histopathology examination finding data of the kidney biopsies of the patients. Neves et al. [82] summated the results as follows:
Neves et al. [82] concluded that their study represents one of the uncommon clinical studies related to Schistosomiasis-associated glomerulopathy with long follow-up and renal endpoints, which had shown that one third of their patients, independent of their histological form, did progress to dialysis.
Gonçalves et al. [83] reported a 36-years-old patient, brown, who had classical symptoms of nephrotic syndrome that included proteinuria greater than 3.5 grams per 24 hours, hypoalbuminemia, and hypercholesterolemia. Nevertheless, in view of a 7-years antecedent history of hepatosplenic history and portal hypertension, he did undergo a biopsy of his kidney and pathology examination of the biopsy specimens demonstrated IgA deposits within the mesangial layer and which were more intense than immunoglobulin G (IgG), that was accompanied by C1q and C3, with 4 out of 13 glomeruli sclerotic, standard light mesangial glomerulonephritis renal injury with IgA deposits. The patient was commenced on angiotensin receptor blocker (ARB) which resulted in progressive improvement with regards to the proteinuria. Gonçalves et al. [83] stated the ensuing:
Gonçalves et al. [83] concluded that:
Dos-Santos et al. [84] made the ensuing summations related to Schistosomiasis of the kidney:
Pallangyo et al. [85] reported a case of massive bilateral hydroureteronephrosis as well as end-stage renal disease which had resulted from chronic Schistosomiasis in a 38-years-old man of African origin. The 38-year-old man was a rice farmer of African origin who had manifested with elevated blood pressure, swelling of his abdomen, as well as reduced urinary output over the preceding 10 months. He had abdominal examination which demonstrated an intra-abdominal mass which had measured 30 cm x 17 cm extended from his right hypochondrium downward to his right inguinal region outward to his umbilicus and crossing the midline. The results of his routine biochemistry and haematology blood test results revealed an estimated glomerular filtration rate of 3.9 mL/min, haemoglobin of 6.78 grams / decilitre, as well as many electrolyte abnormalities. He had computed tomography (CT) intravenous urography scan of abdomen which demonstrated hepatomegaly of 18 cm, bilateral enlargement of kidney with hydroureteronephrosis, multiple calcifications within his urinary bladder. Schistosoma haematobium eggs were isolated examination of his rectal biopsy specimen which confirmed the diagnosis. Pallangyo et al. [85] stated that Schistosomiasis of the urinary tract could be distressing upon the urinary tract system in particular as well as the survival prospects of the patients generally. In view of this observation, it is important that an extensive evaluation of the genitourinary system should form a pivot for the timely diagnosis as well as prompt management of patients especially with regard to residents within Schistosoma-endemic communities who manifest with obstructive uropathy. Pallangyo et al. [85] also made the ensuing iterations:
Duarte et al. [86] stated that kidney involvement in Schistosoma Mansoni infection had not been well studied. Duarte et al. [86] investigated the occurrence of kidney abnormalities in patients who had hepatosplenic schistosomiasis (HSS), especially renal tubular disorders. Duarte et al. [86] undertook a cross-sectional study with 20 consecutive patients who had hepatosplenic schistosomiasis (HSS), who had been followed-up within a Medical Centre in Maceió, Alagoas, Brazil. They performed urinary acidification and concentration tests with utilization of calcium chloride (CaCl2) after 12-hour period of water and food deprivation. They quantified within urine, the biomarker monocyte chemoattractant protein 1 (MCP-1). They calculated the fractional excretion of sodium (FENa+), trans-tubular potassium gradient (TTKG), and solute-free water reabsorption (TcH20). The hepatosplenic schistosomiasis (HSS) group was compared to a group 17 healthy volunteers. Duarte et al. [86] summarized the results as follows:
Duarte et al. [86] made the ensuing conclusions:
Arndts et al. iterated the following summations related to some aspects of Schistosomiasis: [87]
It would be argued that the aforementioned summation has illustrated advances that have been made with regard to the diagnosis of schistosomiasis which would further help with regard to the early diagnosis of schistosomiasis related nephropathy.
Seck et al. [88] reported a 10 year-old boy who was admitted into the nephrology department who had manifested with generalized oedema, hypertension, as well as fatigue over the preceding 3 weeks. He did not have any significant past medical history and he had completed his immunization. His mother did report that he had had baths within stagnant water 5 years earlier in their village. He did not have any personal history or family history of haematuria or oedema. He was found on examination to have a height of 130 cm, and he had weighed 30 kilograms, his temperature was 37 degrees centigrade, his blood pressure was 150/90 mm Hg which was high, he had tachycardia with a heart rate of 100 beats per minute, he had oedema over his face, back, limbs, as well as mild ascites. His Cardiac and pulmonary auscultations were normal. His examination did not demonstrate any evidence of arthritis, or abnormality of his skin. The results of his haematology blood tests were reported as follows (Blood parameter): Red blood cells were 3.4 x 10 12/L; Haemoglobin 9 grams per decilitre; Mean corpuscular volume 85 femtoliters; white blood cells 7.8 x 109/L; Eosinophil count 0.15 x 109/L; Platelet count 300 x 109/L; Blood urea nitrogen 73 mg / dL; Serum creatinine 1.8 mg / dL; Estimated glomerular filtration rate (using original Schwartz formula) 40 mL/min; serum Calcium 7.9 mg / dL; phosphoremia 6.0 mg / dL; Erythrocyte sedimentation rate 45 mm / hr; C-reactive protein 4.0 mg / L; serum protein 45 grams / litre; serum albumin 20 grams / litre. The results of his urinalysis were reported as follows: Proteinuria 254 mg / kilogram / day; Haematuria 23/mm3; Leucocytes in urine 10/mm3; Urine culture – sterile; Schistosoma eggs – absent. The serology examination results of his hepatitis B, C, and HIV tests were negative and his serum complement (CH50) were slightly low. Cryoglobulins, and anti-DNA as well as anti-streptococcal antibodies were not found in his laboratory tests. He had ultrasound scan of the kidneys and lower urinary tracts that were found to be normal. A diagnosis of nephrotic syndrome was rendered and he was treated with utilization of oral prednisolone of 2mg per kilogram per day which was combined with captopril of 50 mg per day, as well as salt-free diet, furosemide of 60 mg per day, and oral supplementation with potassium, calcium, as well as vitamin D3. Four weeks subsequently, his oedema had decreased slightly as well as his urine albumin excretion did slow down at 187 mg / kg / day. His urine sediment was still not remarkable. He received a second 4-week period of oral prednisolone which was started pursuant to three daily intravenous pulses of methylprednisolone 10 mg per kilogram per day. Nevertheless, the results of his clinical and biological findings had not improved at the end of this treatment. He therefore underwent kidney biopsy and pathology examination of the biopsy specimen demonstrated type 1 membranoproliferative glomerulonephritis (MPGN) (see figure 2) with mild tubulointerstitial fibrosis and a granuloma that consisted of histiocytes and giant cells encompassing an egg of Schistosoma Haematobium (see figure 3). Congo red staining of the specimen was negative and immunofluorescence did not reveal any deposition. The results of his circulating IgG antibodies against Schistosoma antigens were high at 1 / 250. A final diagnosis of type 1 MPGN secondary to Schistosoma Haematobium was made. The histopathology examination findings of the kidney biopsy specimens did correspond to Class III-IV of the African Association Nephrology (AFRAN) classification. [71] [89]
Despite the absence of adult Schistosoma worms within the urine and the renal parenchyma of the patient, he received treatment that consisted on praziquantel with 40 mg / kg dose orally to ensure complete cure. After 1 month of this treatment, there was no improvement in the results of his renal function tests. Because of this, oral cyclophosphamide that comprised of 2 mg / kilogram/ day was added to his corticosteroids with supportive treatment that comprised of salt-free diet, captopril, furosemide, calcium, as well as vitamin D3 for a period of 6 months. However, he did reach end-stage renal disease (ESRD) 1 year later and he had to be commenced on haemodialysis.
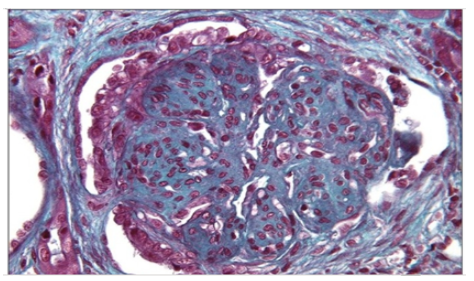
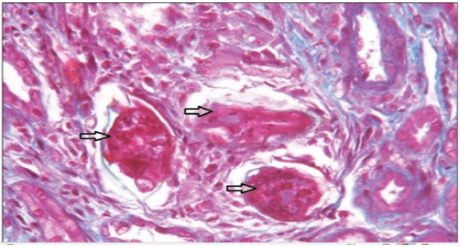
Seck et al. [88] stated the following:
Seck et al. [88] made the ensuing conclusions:
Conclusions and Recommendations
Conflict of Interest Declaration - None
Acknowledgements
Acknowledgements to:
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation. “The peer review process was efficient and constructive, and the editorial office provided excellent communication and support throughout. The journal ensures scientific rigor and high editorial standards, while also offering a smooth and timely publication process. We sincerely appreciate the work of the editorial team in facilitating the dissemination of innovative approaches such as the Bonori Method.” Best regards, Dr. Matteo Bonori.

I recommend without hesitation submitting relevant papers on medical decision making to the International Journal of Clinical Case Reports and Reviews. I am very grateful to the editorial staff. Maria Emerson was a pleasure to communicate with. The time from submission to publication was an extremely short 3 weeks. The editorial staff submitted the paper to three reviewers. Two of the reviewers commented positively on the value of publishing the paper. The editorial staff quickly recognized the third reviewer’s comments as an unjust attempt to reject the paper. I revised the paper as recommended by the first two reviewers.
