
Case Report | DOI: https://doi.org/10.31579/2694-0248/008
*Corresponding Author: Elvis Rafael Ávila Santana, 1First Degree Specialist in Orthopedics and Traumatology. Instructor teacher. William Soler Pediatric Hospital. Havana, Cuba 2020.
Citation: E R Á Santana, E A Santana, L F Barranco, N C Carbalido.(2020). Congenital luxation of the knee: with regard to a case. Clinical Orthopaedics and Trauma Care. 2(1); DOI:10.31579/2694-0248/008
Copyright: ©2020 Elvis Rafael Ávila Santana, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 July 2020 | Accepted: 16 October 2020 | Published: 21 October 2020
Keywords: complex loss of substance; trauma of the large fingers; amputation; fingertip injury; neurovascular flaps
Introduction: the traumatic injuries of the hand are in the top of the list of industrial working accidents. The treatment of these injuries has as goal to restore the function of the fingertip, improving the life quality of the patients.
Objective: to evaluate results of the application of neurovascular homodigital flaps on the cutaneous defects of the digital fingertip of the large fingers of the hand.
Method: it was perform an observational and descriptive type investigation, in a case chain of 33 patients on the Hermanos Ameijeiras Hospital in the period of October 2013 up to January 2015, were it was apply neurovascular homodigital flaps with direct circulation (17 patients) or indirect circulation (16 patients).
Results: male sex was more affected, with a higher frequency between 36 and 41 years old and also over 41 years old. There was confirmed 4 complications representing the 12%. It was obtained a 72.7% of good and excellent results with the application of these surgical techniques getting an appropriate protector sensibility and a satisfactory cutaneous covering. The patients were satisfied in a 93.9% of the cases with the application of these procedures.
Conclusions: it was demonstrated the efficiency of the application of neurovascular homodigital flaps on the cutaneous defects of the digital fingertip of the large fingers of the hand.
The frequency of hand injuries in industrialized countries represents a third of all accidents. Hand injuries are often treated by inexperienced surgeons, which explains a large part of the aftermath after the accident.
There are multiple surgical procedures to treat losses of complex substance from the digital pulp: targeted healing, free skin graft, Kutler and Atasoy flaps, and neurovascularized homodigital flaps. In the center in question, the homo-digitized neurovascularized island flaps are used because the transferred tissue satisfies the requirements of the reconstruction of the pulp, both from the mechanical and the sensitive point of view, providing a satisfactory protective sensitivity to the receptor area without affecting the main sensitivity of the donor finger, which motivated us to evaluate the results of its application taking into account age, sex, type of amputation, production mechanism, occupation and time of evolution and incorporation to work. The main complications of surgical treatment were also determined.
The objective of our research is not to compare methods but to present the results of our experience since the procedures that we apply, in addition to providing adequate skin coverage, provide a satisfactory protective sensitivity to the receiving digital pad.
Material and Methods
The universe of the study was made up of patients with complex loss of substance from the digital pad of the long fingers of the hand from consultations at the “Hermanos Ameijeiras” Clinical-Surgical Hospital. The sample consisted of 33 patients with complex loss of substance from the long fingers of the hand with surgical criteria of monopedicular neurovascularized homodigital flaps on an island, applying direct circulation flaps to 17 patients (Fig. 1) or indirect circulation to 16 patients (Fig. 2).


Inclusion criteria.
1. Patients over 18 years of age.
2. Patients with lesion of the digital pulp with loss of complex substance from the long fingers of the hand (2nd to 5th fingers), zone 2 and 3 of Merle and Dautel.
3. 6-month postoperative follow-up.
4. Acceptance by the patient of the surgical treatment.
Exclusion criteria.
1. Patients with thumb injuries.
2. Patients who refuse surgical treatment.
3. Patients who do not attend scheduled consultations.
4. Patients who voluntarily wish to leave the study.
Criteria for interruption or exit.
1. Patients who abandon outpatient follow-up.
2. Patients who do not comply with medical indications.
Variables
Age, sex, production mechanism, occupation, type of amputation (Obliquity of the cut), interval between injury-operation, surgical technique, incorporation to work and complications.
The evaluation of the results was carried out according to the Excellent, Good, Fair and Bad scales, taking into account: necrosis of the flap, protective sensitivity, discrepancy of two static points (S2PD), discrepancy of two dynamic points (M2 PD), hypertrophic scar in the borders of the donor area, pain, retractable surgical wound scar, total active flexion (total active motion) of the interphalangeal joints (TAM), flexion or extension contracture of the proximal metacarpophalangeal and interphalangeal joints, stiffness and patient satisfaction.
Procedures
General
Patient in supine position on the operating table, the arm is placed on the hand table, asepsis and antisepsis of the hand is performed, field cloths are placed, regional or local anesthesia is applied (2% lidocaine diluted to 1%) and a tourniquet is placed tire for ischemia.
Specific
Direct circulation monopediculate neurovascularized island flap homodigital.
The island is drawn at the distal end of the affected finger to be used to cover the skin defect, a mid-lateral incision is made on the radial side if the affected one is the 2nd or 3rd finger, and the ulnar side if it is the 4th or 3rd finger. 5th. The island flap is released from the flexor sheath. When sectioning the medial side of the flap, it is advisable to carefully haemostasis the arterial vascular arch of the pulp. The perivascular fatty environment of the pedicle must be preserved. The pedicle dissection can be carried proximally up to the level of the commissure. The two anastomotic arches of Edwards must be located and electrocoagulated in the vicinity of the distal metaphysis of the first and second phalanges. The advancement obtained is the product of pedicle dissection and flexion placement of the interphalangeal joints. A flap is placed in the receptor site, fixing it with a percutaneous needle, it will be removed when the flap is sutured with simple stitches, as well as the rest of the surgical wound. The donor site is grafted using intermediate thickness skin, taken from the hypothenar eminence.
Indirect circulation monopediculate neurovascularized island flap homodigital.
The island is drawn at the proximal end of the affected finger (palmar aspect of the first phalanx) that is to be used to cover the skin defect, medial-lateral incision is made on the radial side if the affected finger is the 2nd or 3rd finger and ulnar side if it is the 4th or 5th. After determining the necessary length of the collateral nerve for the flap defect, it is sectioned in the palm, leaving a stump of the nerve surrounded by palmar adipose tissue. The palmar collateral artery is in turn divided between two ligatures on the proximal edge of the island flap. Dissection continues from proximal to distal, individualizing the pedicle, away from the pedicle elements. The dissection is stopped before reaching the neck of the second phalanx, so as not to damage the anastomotic arch that will feed the flap with reverse circulation. The flap is rotated to cover the skin defect. Microsurgical suture is made between the distal end of the healthy contralateral digital nerve and the flap nerve. The flap is sutured with simple stitches at the level of the loss of substance and then the donor site in the first phalanx is grafted using a total skin graft.
Statistical Analysis
In the statistical analysis, summary measures were used for qualitative variables such as percentages and for quantitative variables the mean and standard deviation.
Due to the small sample sizes, the non-parametric Kruskal-Wallis test was used to compare the means of age according to the surgery result, with a significance level of 0.05.
Results
The most affected age group was between 36-41 years, 10 patients (30.3%) followed by those> 41 years, nine patients (27.3%). Average age was 37.3 10.3 years
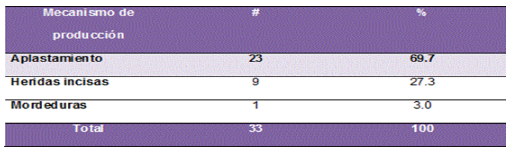
According to the production mechanism, the project showed that the most frequent mechanism was crushing, represented by 23 patients constituting 69.7%. (Table 1)
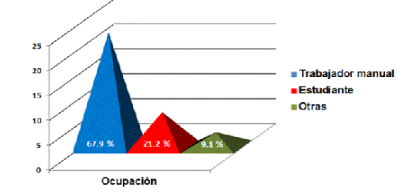
Regarding the occupation of the patients, the most affected were manual workers, 23 patients (69.7%). (Figure 1).
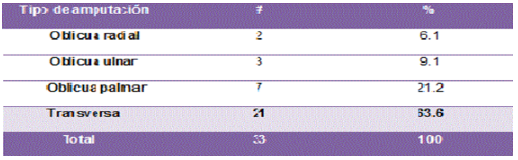
In the series studied, the transverse lesion of the soft foot prevailed, represented by 21 patients (63.6%). (Table 2)
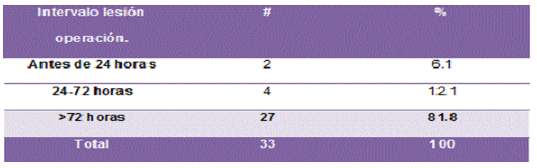
Regarding the time elapsed between the injury and the surgery, the patients operated after 72 hours predominated, 27 patients (81.8%). (Table 3).
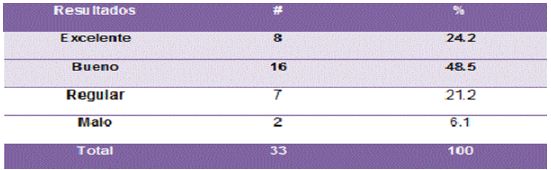
Regarding the final results of the investigation, 24 patients (72.7%) obtained Excellent and Good results. The two patients (6.1%) with poor results presented: 1-) total necrosis of the lame, it was a diabetic patient with more than 30 years of evolution, hypertensive and smoker of more than one box of daily cigarettes 2-) rigidity in flexion of the proximal interphalangeal joint due to lack of physical therapy and poor patient cooperation (Table 5)
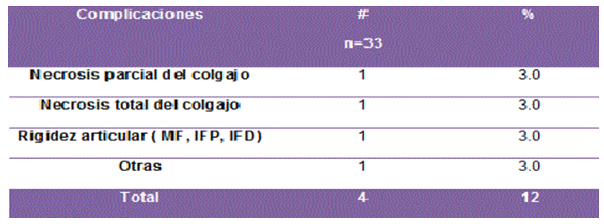
There were 4 complications (12%). The first complication was total necrosis of the flap in a 55-year-old patient, a diabetic with more than 30 years of evolution, hypertensive, and a smoker of more than one box of cigarettes a day. To solve it, we had to perform necrectomy and targeted healing, but the patient lost the possibility of a more adequate skin coverage and a satisfactory protective sensitivity, so he was also unsatisfied as described above. The second complication was a stiffness in flexion of the proximal interphalangeal joint due to lack of physiotherapy and poor patient cooperation, which was resolved with a second surgical procedure where we sectioned the retinacular ligaments on both sides of the proximal interphalangeal joint and also the lateral recesses of the the plate fly. The third complication was partial necrosis of the flap in another 57-year-old patient, a 13-year-old diabetic and alcoholic. Surgical debridement and targeted healing were also performed, but as the necrosis was partial, the rest of the flap showed adequate coverage with satisfactory protective sensitivity without affecting patient satisfaction. The fourth complication was a parrot-beak deformity in a 30-year-old male patient, a baker, who despite the deformity was satisfied because his main objective was to resolve the skin defect with satisfactory protective sensitivity. (Table 6)
According to the literature consulted, these age groups are more likely to present these injuries because in these stages people are more active at work. ([1,2,6] In the fourth decade of life there is a work experience that brings greater confidence when handling work instruments, which causes non-compliance with protection measures. They also decrease the individual's physical aptitudes, such as: visual deficit, incoordination of fine manual movements and a decrease in the ability to react to dangers.
Digital pulp lesions were more frequent in males, represented by 27 patients (81.8%). Coinciding with the series by Adani et al. [7, 11, 20] It is based on the fact that men perform manual activities of greater risk compared to women.
Due to the great industrial development and the incorporation of multiple complex heavy machinery, crush trauma and blunt avulsive wound are more frequent than incised wounds and bites. Frank Fang et al. [9, 10, 13] and Carlos E. [8, 13] agree with our report.
With the increase in industry and the mechanization of work tools, the manual worker, by the nature of his trade, traumatizes his hands. Hands top the list for industrial workplace accidents and are responsible for much of the compensation costs. [1, 3, 15] French annual statistics report 360,000 hand accidents (32% of work accidents). [17, 18, 19, 21]
Frequently, the production mechanisms that cause these injuries contribute to great contamination of the wounds that also occasionally become well established around 72 hours. Godina [4] recorded an incidence of infection of 1.5% using a protocol of excision of the lesion and skin coverage by microsurgery in 72 hours and an incidence of infection of 17.5% with the closure of the wound in less than 72 hours. Lister and Schoker [4] presented satisfactory results using skin coverage through the use of flaps in the 24 hours following the injury. Brenner et al. They did not observe significant differences in infection rates when they compared emergency primary transfer of free and / or vascularized tissue versus delayed primary or secondary transfer. Delayed treatment allows the injury to be evaluated a second time, verifying the viability of the limb in order to plan the intervention more precisely. However, in our series, no infection was found before or after 72 hours. [4, 12, 16]
Bunelli F. [14, 15, 22] demonstrated in her research that the described incorporation fluctuated between 5-6 postoperative weeks, while the cases incorporated in the two series after eight weeks were those that presented complications. Incorporation before four weeks is difficult when more complex surgical techniques are applied since healing and rehabilitation require at least one month of evolution to obtain a satisfactory result.
The different studies reviewed coincide with our investigation and the results obtained in the present investigation. S. Rojas Sabapathy and Godina [4] demonstrated excellent results with the use of homodigital neurovascularized flaps in covering the loss of complex substance from the pulp.
According to Merle [3, 5] the most frequent complications are: total and partial necrosis of the flap and stiffness of the metacarpophalangeal, proximal and / or distal interphalangeal joints, coinciding with what has been reported by several authors. The study yielded similar results to those obtained in the literature.
Conclusions
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
