
Research Article | DOI: https://doi.org/10.31579/2640-1045/008
*Corresponding Author: Shereen Abdelghaffar, Professor of Pediatrics, Pediatric Endocrinology and Diabetes , Ethiopia.
Citation: Shereen Abdelghaffar, Mohamed A Ghoneim, Mohamed Adel el-Masry, Ashraf F Nabhan, Ashraf Anas Zytoon. Primary Congenital Hypothyroidism: Pharmacokinetics of Levothyroxine for the Treatment of Hypothyroidism. J. Endocrinology and Disorders. Doi:10.31579/2640-1045/008
Copyright: © 2017. Shereen Abdelghaffar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 June 2017 | Accepted: 19 July 2017 | Published: 10 August 2017
Keywords: Neonatal screening, congenital hypothyroidism, iodine deficiency.
Primary congenital hypothyroidism (CH) is a condition that affects the body's thyroid gland, a small organ in the lower neck. People with CH are unable to produce enough thyroid hormone, a chemical that is essential for healthy growth and development.
If left untreated, CH can cause sluggishness, slow growth, and learning delays. However, if detected early and treatment is begun, individuals with CH often can lead healthy lives.
Most neonates born with CH have normal appearance and no detectable physical signs. Hypothyroidism in the newborn period is almost always overlooked, and delayed diagnosis leads to the most severe outcome of CH, mental retardation, emphasizing the importance of NS. Blood spot thyroid stimulating hormone (TSH) or thyroxine (T4) or both can be used for CH screening. The latter is more sensitive but not cost-effective, so screening by TSH or T4 is used in different programs around the world. TSH screening was shown to be more specific in the diagnosis of CH. T4 screening is more sensitive in detecting especially those newborns with rare hypothalamic-pituitary-hypothyroidism, but it is less specific with a high frequency of false positives mainly in low birth weight and premature infants. The time at which the sample is taken may vary. In the majority of the centers, blood is obtained from a heel prick after 24 hours of age to minimize the false positive high TSH due to the physiological neonatal TSH surge that elevates TSH levels and causes dynamic T4 and T3 changes in the first 1 or 2 days after birth. Early discharge of mothers postpartum has increased the ratio of false positive TSH elevations. Although transient hypothyroidism may occur frequently, all these infants should be treated as having CH for the first 3 years of life, taking into account the risk of mental retardation. A reevaluation after 3 years is needed in such patients. The goal of initial therapy in CH is to minimize neonatal central nervous system exposure to hypothyroidism by normalizing thyroid function, as rapidly as possible.
As is often the case with older drugs, the pharmacokinetics of levothyroxine is often under-appreciated or misunderstood and many factors influence the optimal dosing of levothyroxine.
Congenital hypothyroidism (CH) is the most common congenital endocrine disorder in childhood and also is one of the most common preventable causes of mental retardation. After making diagnosis if the treatment is started within in a few weeks of birth, neurodevelopmental outcome is generally normal. The clinical features of congenital hypothyroidism are often subtle and many newborn infants remain undiagnosed at birth. This is due in part to passage of maternal thyroid hormone across the placenta providing a protective effect, especially to the fetal brain and masking the clinical signs. Also, even the most common forms of CH have some moderately functioning residual thyroid tissue making clinical diagnosis difficult. Within few weeks of birth as hypothyroxinemia progresses clinical signs and symptoms of hypothyroidism become more obvious and put neonatal brain at risk of irreversible injury. Because of this danger, it is important to start treatment as soon as possible after birth. For all of the above reasons, screening has become the best way to detect infants with CH in many parts of the world. Pilot screening programs for CH were developed in Quebec, Canada and Pittsburgh, Pennsylvania in 1974 and have now been established in Western Europe, North America, Japan, Australia and parts of Eastern Europe, Asia, South America and Central America. As Indian data are lacking, In North America, more than 5 million newborns are screened and approximately 1400 infants with CH are detected annually.
Newborn screening (NS) for CH is one of the major achievements of preventive medicine. Although since 1972 the problem of CH has been resolved in developed countries by the implementation of NS, the same cannot be said for developing countries that still have no NS programs for CH. Since diagnosis based on clinical findings is delayed in most instances because of few symptoms and signs, hypothyroidism in the newborn period is almost always overlooked, and delayed diagnosis leads to the most severe outcome of CH, namely, mental retardation. In a Danish study conducted on infants born between 1970 and 1975, it was emphasized that only 10% of the affected infants were diagnosed within the first month of life, 35% within 3 months, and 70% within the first year. In the remainder of the infants, the diagnosis was delayed to the 3rd and 4th years of life. In a retrospective analysis of 1000 cases of CH from Turkey, the mean age at diagnosis was reported to be 49 months, and only 3.1% of cases were diagnosed within the first month, while 55.4% were diagnosed after 2 years of age.
Epidemiology
The overall incidence of CH ranges from 1 in 3000 to 1 in 4000 newborn infants. The incidence of CH is higher in Hispanic and Asian individuals and lower in black individuals. There is a 2:1 greater incidence in females compared with males and there is an increased risk in infants with Down's syndrome. In India, the prevalence has been reported to be 1 in 2640 in screening 40,000 newborn. In 2007, Harris and Pass reported that the incidence (birth prevalence) of CH detected by newborn screening programs in the United States had nearly doubled over the previous two decades, increasing from 1:3985 (in 1987) to 1:2273 (in 2002).
Etiology
In the majority of patients, CH is caused by an abnormal development of the thyroid gland (thyroid dysgenesis) which is usually a sporadic disorder and accounts for 85% of cases. It presents in three major forms i.e. thyroid ectopy, athyreosis and thyroid hypoplasia. Thyroid ectopy accounts for two thirds of cases of thyroid dysgenesis and is twice more common in females. The exact etiology of thyroid dysgenesis is not known. However; mutations in transcription factor genes that regulate thyroid gland development [thyroid transcription factor 2 (TTF-2), NKX2.1 (also termed TTF-1) or PAX-8] would explain these defects. But, only 2% of cases with thyroid dysgenesis are found to have such genetic mutations.
Diagnostic evaluation
In countries where newborn screening programs take place, all infants with CH are diagnosed after detection by newborn screening tests. However, of the worldwide birth population of 127 million, only 25% of babies are invited for screening for CH. For the remaining 75% infants, particularly concentrated in developing countries, clinical suspicion of hypothyroid leads to thyroid function evaluation.
The ideal time to obtain the blood spot is 3-5 days after birth to minimize the false positive high TSH values due to the physiological neonatal TSH surge that elevates TSH levels and causes dynamic T4 and total triiodothyronine (T3) changes in the first 1 or 2 days after birth. Early discharge of mothers postpartum has increased the ratio of false positive TSH elevations from 3:1 to 5:1. The difficulty in screening for CH using cord blood samples is with the handling and transporting the samples, making it an impractical method for mass screening.
In some laboratories, the threshold cut-off is adjusted based on the age of the infant when the blood spot is obtained. The cutoff for reporting an elevated TSH is a level above 20 to 25 mU/mL in most screening programs. Whichever method is used, babies whose initial TSH is >50 mU/mL are most likely to have permanent CH, whereas a TSH level between 20 and 49 mU/mL is frequently a false positive or represents transient hypothyroidism. Transient CH is particularly common in premature infants in borderline iodine-deficient areas.
Newborn thyroid screening protocols
Newborn thyroid screening tests are carried out before discharge from hospital, optimally between 2 and 5 days of age. Specimen collected before 48 h of age may lead to false positive result. Screening of very sick newborn or after blood transfusion may lead to false negative result.
In a critically ill infant or preterm neonate, or in case of home delivery, blood sample should be collected by 7 days of age. Capillary blood samples from heel prick are placed on circles of specialize filter paper, dried at room temperature, then sent to a centralized laboratory. Some programs obtain a routine second specimen between 2 and 6 week of age. The additional incidence of CH based on a second screening at 2 weeks of age is approximately 1 in 30 000.
Earlier for screening of newborn for CH, most programs undertook an initial T4 test, followed by TSH testing if the T4 value falls under a cut off limit. With increasing accuracy of TSH assays on small blood volumes, many screening programs now have switched to an initial TSH test approach to detect CH. Each program should develop its own T4 and TSH cut off for test result. Both methods allow detection of the majority of infants with CH but each approach has its own advantages and disadvantages. The initial T4 then follow up TSH approach will detect some cases of secondary or central hypothyroidism and infant with "delayed TSH elevation". On other hand initial TSH approach will detect mild or subclinical forms of hypothyroidism. Generally, if the screening T4 value is below the 10 th percentile of cut off and/or the TSH is greater than 30mU/liter (15mU/liter whole blood), an infant should be recalled for confirmatory serum testing. In cases with "intermediate results," e.g. low T4 but TSH below cutoff, a program may recommend that a repeat heel prick screening specimen be collected and sent for analysis.
Confirmatory serum thyroid testing
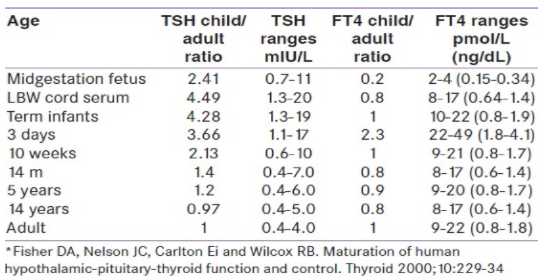
Diagnosis and treatment should not be based on screening test results alone. Neonates with abnormal thyroid screening tests should be recalled immediately for examination and a venipuncture blood sample should be drawn for confirmatory serum testing. Confirmatory serum should be tested for TSH and free T4, or total T4 combined with some measure of binding proteins such as a T3 resin uptake. Serum TSH and T4 undergo dynamic changes in the first weeks of life; it is important to compare the serum results with age-related reference values. [21] In the first few days of life, serum TSH can be as high as 39mU/L, because of the TSH surge that is normally seen after birth. Most confirmatory serum tests are obtained within one to two weeks of age, when the upper TSH range has fallen to an approximately 10mU/liter. Although levels of all hormones are higher at 1-4 days of age, by 2-4 weeks of age they have fallen closer to the levels typically seen in infancy.
Low T4 and elevated TSH values
A low total T4 or free T4 level in the presence of an elevated serum TSH level confirms the diagnosis of primary hypothyroidism. Replacement therapy with levothyroxine (L-T4) should be initiated as soon as confirmatory tests have been drawn before the results of the confirmatory tests are available. Infant with an elevated serum TSH level and a normal free T4 or total T4 is consistent with the diagnosis of subclinical hypothyroidism.
Normal T4 and elevated TSH values
Infant with an elevated serum TSH level and a normal free T4 or total T4 have either a transient or permanent thyroid abnormality or delayed maturation of the hypothalamic-pituitary axis. There is controversy regarding the need for L-T4 therapy in this setting. As TSH concentration is the most sensitive indicator of hypothalamic-pituitary- thyroid axis. A persistent basal TSH concentration higher than 10mU/L (after the first 2 weeks of age) is considered to be abnormal. Therefore, if the TSH elevation persists, the infant should be treated. If such infants are not treated, measurement of FT4 and TSH should be repeated at 2 and 4 weeks and treatment should be initiated promptly if the FT4 and TSH concentrations have not normalized.
Low T4 and normal TSH values
The low T4 with normal TSH profile may result from hypothalamic immaturity particularly in preterm infants, during illness, in central hypothyroidism or in primary hypothyroidism and delayed TSH elevation. There are no clear-cut guidelines regarding follow-up of such patient, to follow-up with serial filter-paper screening tests until the T4 value becomes normal, or to request a second blood sample for measurement of FT4 and TSH. Most infants with low T4 and normal TSH have normal FT4 values and the subsequent thyroid function test results are normal. Treatment of these infants (with the exception of those with central hypothyroidism) with L-T4 has not yet been shown to be beneficial.
Diagnostic studies to determine an underlying etiology
once the diagnosis of CH is confirmed, treatment should never be delayed pending the determination of etiology. Additional studies to determine the underlying cause may be done. But these studies are complimentary as these diagnostic studies do not alter treatment decision.
Pharmacokinetics of Levothyroxin
Levothyroxine (l-thyroxine) tablet is crushed and mixed with breast milk, formula or water and resultant suspension is squirted into cheek pad or can put on open nipple for infant to feed. Various substances interfere Levothyroxine (l-thyroxine) absorption through gut, such as calcium and iron preparation, soy protein formula, sucralfate, aluminium hydroxide and cholestyramine should not be given together. Although, recommendation is to take Levothyroxine (l-thyroxine) empty stomach but for infant it may not be possible.
Dosages
The goal of therapy is to normalize T4 within 2 weeks and TSH within one month. In one study infants who took longer than 2 weeks to normalize thyroid function had significantly lower cognitive, attention and achievement scores than those who achievement scores than those who achieved normal thyroid function at 1 or 2 weeks of treatment. As an optimal neurological development depends on both adequacy and timing of treatment, American academy of pediatrics and European society of pediatric endocrinology recommend 10-15 μgm/kg/day as initial dose. Studies show that this dose normalizes serum T4 within 3 days and TSH within 2-4 weeks. Initial LT4 dose and rapid normalization of serum T4 are critical to the optimal neurodevelopmental outcome. In severe CH, it is important to start higher initial dose of the recommended range to achieve these goals. In one study infants who started on higher initial doses 50μgm had full-scale IQ scores 11 points higher than those started on lower initial doses 37.5 μgm.
Target concentrations
Guidelines of American academy of pediatrics and European society for pediatric endocrinology recommend that T4 concentrations should be kept in the upper half of reference range. Target values for T4 are 10-16 μgm/dl; FT4 1.4-2.3ng/dl and TSH <5 μU/dl (optimally 0.5-2.0 μU/dl) for first 3 years of life. Thereafter, T4 should be kept in the upper half of normal range.
One study showed lower IQ in infants with T4 concentration below 10 μgm/dl during first year of life along with TSH above 15 μU/dl compared with those having T4 concentrations more than 10 μgm/dl. Higher doses of Levothyroxine (l-thyroxine) have been associated with better intellectual outcome in children with CH. However, some studies have shown that higher doses of Levothyroxine may result in behavior problems like increased anxiety, social withdrawal and poor concentration at age of 8 years demonstrating thus potential dangers of overtreatment with levothyroxine in CH children.
Congenital hypothyroidism (CH) is one of the most common preventable cause of mental retardation. The best way to detect infants with CH is by screening large populations of newborns. If the diagnosis is made and treatment started within a few weeks of birth, neurodevelopmental outcome generally is normal. The etiology of the most common cause of CH, thyroid dysgenesis, is largely unknown as the increase incidence of CH.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
