
Research Article | DOI: https://doi.org/10.31579/2692-9562/126
1ENT department. Military hospital of Tunis. Tunisia
2University of El Manar. Tunis. Tunisia
*Corresponding Author: Sameh Mezri, ENT department. Military hospital of Tunis. University of El Manar, Tunis. Tunisia.
Citation: Sameh Mezri, Haddaji Meriem, Gharsalli Jihène, (2024), Predictives Factors of Surgical Failure in Secondary Hyperparathyroidism, Journal of Clinical Otorhinolaryngology, 6(5); DOI:10.31579/2692-9562/126
Copyright: © 2024, Sameh Mezri. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 26 June 2024 | Accepted: 05 July 2024 | Published: 11 July 2024
Keywords: renal insufficiency; secondary hyperparathyroidism; parathyroidectomy; surgical failure
Background:
Secondary hyperparathyroidism is the main metabolic bone disorder related to chronic kidney disease characterized by hypersecretion of parathormone (PTH). Given the high cost and the unavailability of calcimimetics based treatment, surgery still represents the best available treatment option.
Our objectives were to evaluate surgical outcomes of parathyroidectomy (PTX) in terms of efficacity and risks factors associated to postoperative complications and failure in order to deduce the precautions to take for better results.
Methods: This was a retrospective study including 45 patients undergoing surgery over a period from 2019 to 2021. Our analytical study has defined predictive criteria of surgical results and postoperative complications, with a threshold significant < 0.05.
Results:
The average age of patients was 46 years with a sex ratio of 1.5. Mean preoperative biological parameters value was 2030 ng/L for PTH, and 2,4 mmol/L for corrected calcemia. We underwent subtotal PTX (7/8) in 25 cases, selective PTX (3/4) in 15 cases. Five patients had incomplete surgery. Reporting to KDOQI 2003 criteria, surgical success rate reached 87% with a mean postoperative value of PTH of 202.5 ng/L. Subtotal PTX was related to better surgical results. However, 38 patients developed postoperative hypocalcemia which was severe in 47% of cases, and 13 patients developed a Hungry Bone Syndrome. High preoperative alkaline phosphatase (> 500 UI/L) and preoperative hypocalcemia were respectively the two main predictive factors of the occurrence of these complications (p<0.05). Postoperative hypoparathyroidism was diagnosed for 11 patients. Severe hypocalcemia (p=0.017) was found to be the predictive factor for its occurrence.
Conclusion:
Although it is more associated with the occurrence of postoperative hypocalcemia, subtotal PTX seems to be more efficient than selective PTX. However, the identification of risk factors and taking the adequate preoperative measures would prevent postoperative complications and grant better surgical outcomes.
Secondary hyperparathyroidism (HPTS) is a common complication of chronic kidney disease (CKD), with a prevalence estimated at 30 to 50% of CKD patients at the dialysis stage [1]. HPTS affects patients' life quality due to complications related to the excess of parathyroid hormone (PTH). The introduction of calcimimetics aimed to alleviate these complications and reduce the need for surgery. However, due to the unavailability of these medical means in Tunisia, making it difficult to achieve the goals of CKD management [2], surgery, particularly parathyroidectomy (PTX), with its various approaches, became the best available means to improve biological parameters and reduce morbidity and mortality associated with HPTS. The aim of this study was to evaluate, based on patient characteristics and surgical technique, the outcomes of surgery for HPTS in terms of efficacy and iatrogenic complications.
We conducted a retrospective study including patients who underwent primary surgery for secondary hyperparathyroidism (HPTS) with chronic kidney disease (CKD) during the period [2019-2021]. We included adult patients (age >18 years) who had been on dialysis for more than six months. We excluded patients with a history of cervical surgery and/or irradiation, those on hemodialysis for less than six months, unexploitable records, and patients without postoperative follow-up or lacking an anatomopathological report. Surgical
Indication: The surgical indication was based on the criteria of the "Kidney Disease Outcomes Quality Initiative (KDOQI) 2003:
Surgical Technique:
Two techniques of parathyroidectomy (PTx) were performed in our series:
Forty-five patients underwent surgery during the study period, with an average age at the time of surgery of 45 years and a sex ratio of 1.5. The average duration of dialysis for our patients was nine years, ranging from two to 18 years. Hypertensive nephropathy was the most common cause of CKD (38%), and in over 40% of cases, the initial nephropathy was not identified. The predominant presenting symptom was bone pain (Table I).
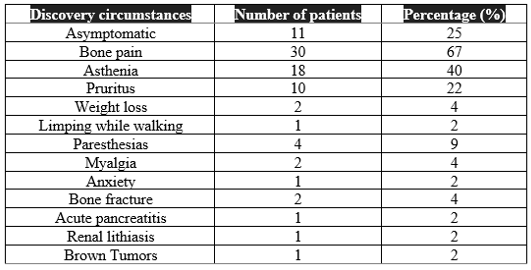
Table I: Circumstances of discovery of SHPT
In terms of laboratory findings, the majority of our patients had normocalcemia (58%), while 18% had hypercalcemia, with an average corrected calcium level of 2.40 mmol/L [range: 1.98-3.30]. Preoperative PTH values ranged from 669 to 5522 ng/L with an average level of 2030 ng/L. All patients had elevated alkaline phosphatase (PAL) levels (average 7 times the normal range). Forty percent (40%) had vitamin D deficiency, supplemented with active vitamin D or UnAlpha® (alfacalcidol) at daily doses ranging from 0.25 to 2 µg. Except for patients with hypercalcemia, all patients received phosphate chelation therapy with calcium-based phosphorus binders.
Preoperative ultrasound data were as follows (Table II).

Table II: Ultrasound Evaluation of patients
Parathyroid glands were not visualized in 39% of cases.
Only 11 patients (24%) underwent dual-phase parathyroid scintigraphy, which revealed an adenomatous appearance of a single gland in five patients (45%), while a hyperplastic appearance of multiple glands was noted in the remaining cases. A single cervico-thoracic CT scan was performed, revealing the presence of brown tumors in the ribs and spine.
Intraoperatively, all four parathyroid glands were identified in 91% of patients (41 cases). In the remaining cases, two patients each had two and three parathyroid glands identified. No ectopic parathyroid glands were found.For surgical choice, subtotal 7/8 PTx was chosen for 25 patients (56%), while selective 3/4 PTx was chosen for 15 patients (33%). Surgery was deemed incomplete in the remaining cases (5 patients). Thyroid surgery was associated in 04 patients; two lobectomy-isthmectomy, one with central lymph node dissection, and two total thyroidectomies. Frozen section examination was performed for all patients, with an anatomoclinical discordance observed in two cases, where the parathyroid nature of one of the three resected glands was refuted. For the thyroidectomy specimens, only one frozen section examination was inconclusive, and the final examination revealed a focus of papillary microcarcinoma. Histopathological examination of the resected parathyroid glands revealed diffuse hyperplasia (67%), nodular hyperplasia (31%), and a parathyroid adenoma (2%) in a patient who underwent incomplete surgery by resecting a single parathyroid gland.
Postoperatively, the PTH level was below 300 ng/L in 39 cases (87%) (Figure 2). Among them, 25 underwent subtotal PTx, 12 underwent selective PTx, and two had incomplete surgery.
For patients with failed initial surgery (six cases), two underwent reoperation after parathyroid scintigraphy. Monitoring was chosen for the other patients (postoperative PTH between 317 and 390 ng/L). Hypocalcemia was the most frequent postoperative complication. Eighteen patients experienced severe hypocalcemia, with 14 following subtotal PTx (77%). Hungry bone syndrome (HBS) was observed in 13 cases (29%), among which nine patients underwent subtotal PTx (70%). Subtotal surgery was associated with the highest incidence of postoperative hypoparathyroidism in our patients (73%). At a later stage, persistent hyperparathyroidism was noted in seven patients, three of whom had initially satisfactory surgical outcomes. We conducted a statistical study to determine prognostic factors for surgical outcomes and postoperative complications. Exploration of more than three confirmed PTGs during frozen section examination and subtotal PTx were associated with surgical success with statistical correlation of (p=0.002) and (p=0.003), respectively, while exploration of fewer than 3 PTGs intraoperatively and incomplete surgery were associated with surgical failure (p=0.001).
Preoperative hypocalcemia, very high preoperative PAL levels, subtotal PTx, postoperative hypoparathyroidism, hypocalcemia on postoperative day 3, and IV correction of hypocalcemia were correlated with the occurrence of HBS. For patients with postoperative hypoparathyroidism, 73% had severe hypocalcemia (p=0.01) and 82% required IV correction (p=0.03). A longer hospital stay was associated with the occurrence of complications, primarily HBS (p < 0 xss=removed>
At three months post-surgery, the PTH levels ranged from 14 to 1008 ng/L, with an average of 308.9 ng/L. Persistent hyperparathyroidism was noted in 7 patients.
Although there is no clear consensus regarding the preoperative protocol, preoperative preparation can reduce post-PTx complications, particularly hypocalcemia. Ho et al. [3] reported that preoperative supplementation with active vitamin D analogs reduces postoperative calcium and vitamin D supplementation requirements. Several factors have proven to be involved in the success of the surgical procedure; preoperative cervical ultrasound coupled with sestaMIBI scintigraphy, surgeon experience, surgical exploration of all four PTGs, and choice of surgical technique. [4] Indeed, the choice of surgery for the treatment of SHPT remains controversial. Several studies have compared total and subtotal surgery in terms of surgical outcomes and postoperative complications. A study published in 2018 showed that mortality and pathological fractures outcomes were comparable. The risk of cardiovascular events was lower in patients undergoing subtotal surgery. Additionally, total surgery was associated with lower postoperative PTH levels and a lower frequency of reoperation [5]. Others suggest that 3/4 PTx represents a fairly effective alternative with less morbidity, fewer permanent hypoparathyroidism cases, and shorter hospital stays than subtotal surgery [6]. There are still some teams that opt for total surgery without autotransplantation and without systematic bilateral thymectomy as another alternative with a lower long-term recurrence rate of SHPT [7]. Recently, guided resection may be a valid choice, reducing operative time while effectively resecting parathyroid adenomas, reducing recurrence or recurrence of HPTS remotely [4]. Perioperative PTH measurement is a fairly reliable technique that guides surgical intervention and should be common practice. In our series, subtotal PTx was performed in 56% of cases, while selective PTx was chosen in 15 patients (33%). Subtotal PTx was associated with successful surgical outcomes in 100% of cases, whereas incomplete surgery was identified as a predictive factor for surgical failure (p=0.001).
In terms of complications, parathyroid surgery in chronic kidney disease patients presents a notable postoperative mortality rate ranging from 1 to 3% within the first 30 postoperative days [8]. This is mainly due to cardiovascular complications and severe hypocalcemia with its cardiac and respiratory impact [9]; only one of our patients died from cardiorespiratory arrest on postoperative day 1. Postoperative hypocalcemia is the most common complication after HPTS surgery [10]. Its incidence is estimated at 72-92
The decision for surgery in cases of secondary hyperparathyroidism (HPTS) due to chronic kidney disease should be made through close collaboration between the nephrologist and the surgeon. Surgery remains the only definitive treatment for the disease, with subtotal parathyroidectomy and total parathyroidectomy with autotransplantation being the two most recommended techniques. However, more conservative approaches may be considered in specific cases. Preoperative topographic assessment, along with comprehensive biological evaluation and correction of metabolic disturbances, are essential to ensure surgical success and prevent complications.
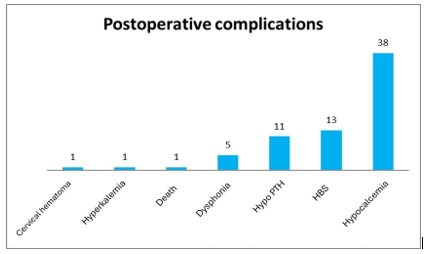
Figure 1: Summary diagram of intraoperative exploration and surgery performed for our patients
Figure 2: Evolution of parathyroid hormone (PTH) levels pre- and postoperatively
Figure 3: Bar chart representation of postoperative complications in patients
The authors declare no competing interests
Informed Consent: Written informed consent was obtained from patients for participate in the study and publish its results. Local ethical comittee of Military hospital of Tunis (Tunisia) have also provided the conduction of the study and authorized the publication of results.
Grant Information: The authors declared that no grants were involved in supporting this work.
Data availability: No data are associated with this manuscrit.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
