
Clinical Images | DOI: https://doi.org/10.31579/2768-2757/103
1 PGY2 Resident, Department of General Surgery, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences University (Deemed University), Wardha, Maharashtra, India.
2 Professor, Department of General Surgery, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences University (Deemed University), Wardha, Maharashtra, India.
3 Professor, Department of Pathology, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences University (Deemed University), Wardha, Maharashtra, India.
4 Professor, Department of Medicine, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences University (Deemed University), Wardha, Maharashtra, India.
*Corresponding Author: Tapesh Dutt Nagaria, PGY2 Resident, Department of General Surgery, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences University (Deemed University), Wardha, Maharashtra, India.
Citation: Acharya S., Shukla S., Shinde R., Tapesh D Nagaria., (2024), Posterior Urethral Valves Leading to Massive Hydronephrosis in A Four-Day Old Babys, Journal of Clinical Surgery and Research, 5(1); DOI:10.31579/2768-2757/103
Copyright: © 2024, Tapesh Dutt Nagaria. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 November 2023 | Accepted: 08 December 2023 | Published: 15 January 2024
Keywords: congenital disorder; diagnosis; cystourethrogram
Posterior urethral valves (P.U.V.s), also referred to as congenital obstructing posterior urethral membranes (C.O.P.U.M.) is a congenital malformation affecting males where the membranous folds of the urogenital membrane obstruct the membranous and prostatic urethra. It is a congenital disorder only seen in males, with an incidence of 1 per 4000 to 1 per 25000 live births in some areas. Type 1 P.U.V. results from the abnormal insertion and absorption of the distal Wolffian duct during the development of the bladder. Type 3 PUV is observed as a membrane in the posterior urethra, originating from the incomplete canalisation between the anterior and the posterior urethra. Type 2 P.U.V. is now considered a normal anatomical variant. Regardless of the type, P.U.V.s present with urinary tract obstruction, bladder distension, abdominal distension, difficulty voiding, poor stream of urine, recurrent Urinary Tract Infection (U.T.I.), diurnal enuresis and a failure to thrive. They are diagnosed Antenatally by Ultrasonography showing distended or thick-walled bladder, bilateral hydroureters, and bilateral hydronephrosis. However, the gold standard for the diagnosis is a Micturating CystoUrethrogram (MCU), also known as a Voiding Cystourethrogram (V.C.U.) shows dilation/elongation of the posterior urethra during voiding along with signs of vesicoureteral reflux if present. This patient was antenatally diagnosed with posterior urethral valves at seven months of fetal age and came to us for further management. Antenatal diagnosis of Posterior Urethral Valves on Ultrasonogram involves visualisation of 1. Keyhole sign- due to the distension of the urethral proximal to the valves and a distended bladder, 2. marked distention or hypertrophy of the bladder, 3. Hydronephrosis and hydroureter. An Ultrasonogram of the abdomen and pelvis done postnatally revealed bilateral gross hydroureteronephrosis, which was missed on antenatal scans. The baby was born to a G2P1L1 mother and weighed 3.04kg at birth. The baby cried immediately after birth and maintained oxygen saturation at 100% on room air. The patient was managed with Cystoscopy with Posterior Urethral Valve fulguration with circumcision.

Figure 1: a Micturating Urethrogram showing bilateral grossly dilated ureter and renal pelvis along with posterior urethral valve as a narrowing in the posterior urethra.
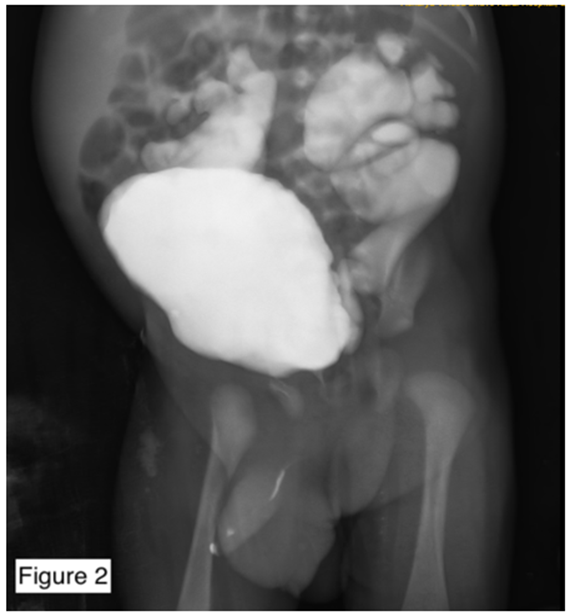
Figure 2: A Micturating Urethrogram - Lateral view - showing bilateral grossly dilated ureter and renal pelvis along with posterior urethral valve as a narrowing in the posterior urethra.
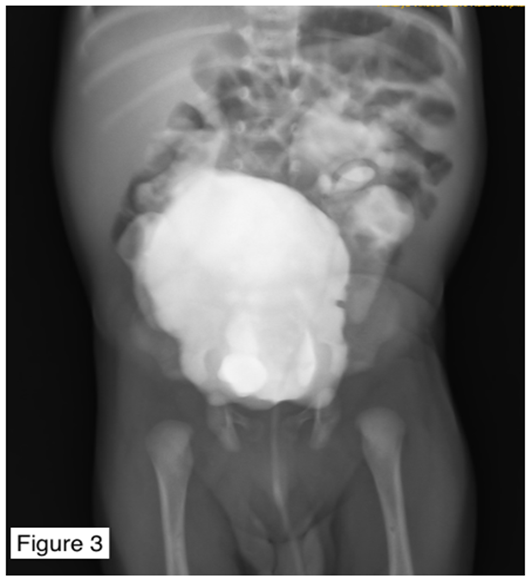
Figure 3: A Micturating Urethrogram - showing filled-up urinary bladder.
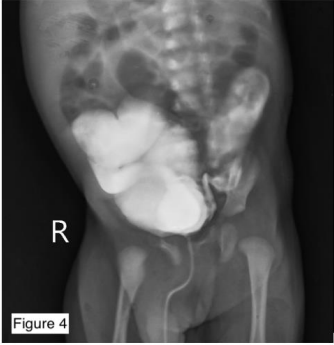
Figure 4: A Micturating Urethrogram - Lateral view - showing bilateral grossly dilated ureter and renal pelvis along with posterior urethral valve as a narrowing in the posterior urethra.
Bilateral Grade V Hydronephrosis with Posterior Urethral Valves
Differential Diagnosis-
Urethral Stricture
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
