
Research Article | DOI: https://doi.org/10.31579/2690-8794/099
*Corresponding Author: Jose A. Pinto Tasende, MD, PhD, Department of Rheumatology-INIBIC, Complexo Hospitalario Universitario de A Coruña, 84 Xubias de Arriba Road, 15006 A Coruña, Spain.
Citation: Jose A. Pinto Tasende Jose M. Lorenzo Alvarez, Carlota Iñiguez Ubiaga, Luis Fernández Dominguez, Carlos García Porrúa, Francisco J. Maceiras Pan, Jose L. Guerra Vázquez and Jose A. Mosquera Martínez (2021) Obesity and Clinical Activity in Psoriatic Arthritis Patients Treated with Synthetic Disease-Modifying Antirheumatic Drugs. J, Clinical Medical Reviews and Reports. 3(9); DOI: 10.31579/2690-8794/099
Copyright: © 2021, Jose A. Pinto Tasende, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 August 2021 | Accepted: 13 September 2021 | Published: 30 September 2021
Keywords: corticosteroid; csDMARD; DAPSA score; enthesitis; metabolic syndrome; obesity; psoriatic arthritis
Introduction: Comorbidities are prevalent in psoriatic arthritis (PsA) and which may affect disease activity and response to therapy.
Aims: To evaluate comorbidities among patients with PsA naïve to biologics, and their association with basal inflammatory activity status, before starting them.
Methods: We performed a retrospective cross-sectional a study of cohort of patients with PsA (CASPAR criteria), treated with synthetic disease-modifying antirheumatic drugs. Patients were managed according to EULAR/GRAPPA recommendations, and the collected variables included demographics, clinical, serological, classical CV risk factors, and treatment. Disease activity was assessed using the Disease Activity Score for Psoriatic Arthritis and clinical DAPSA scores. The tests were two-tailed, with a significance level of <0.05.
Results: A total of 416 patients were included in the study: 222 maintained remission or low disease activity being treated without biologics, and 194 who needed to be treated with bDMARD because they did not response well to csDMARD. From patients who were waiting to start biologics, 38.1% had obesity and had increased risk of MetS for age > 50 years old (OR 3.287 [95%CI: 1.258-8.591], p 0.015) and CRP > 0.5 mgr/dL (OR 2.684 [95%CI: 1.141-6.313], p 0.024) but not for cDAPSA>13 (OR 1.539 [95%CI: 0.695-3.409], p 0.288).
DAPSA score was higher in patients with obesity, 20.3 (14.4) vs 13.8 (8.5), p0.010 and these patients had an OR for cDAPSA>13 of 3.15 [95%CI: 1.07-9.25], p 0.037). Patients with obesity had a higher frequency of DAPSA and cDAPSA MoDA-HDA (p = 0.022; p = 0.032). In the linear logistic regression analysis, a high-moderate DAPSA score was associated with obesity (p = 0.017), CRP (p <0.0001), and cDAPSA score with obesity (0.029) but not with CRP (p = 0.748). Obesity and corticosteroid treatment were independent factors for cDAPSA>13 and the presence of enthesitis for cDAPSA≤13.
Conclusion: PsA patients who did not respond well to csDMARD had a higher prevalence of MetS, associated with age > 50 years and CRP higher than normal values. The DAPSA score was higher in patients with obesity and corticosteroid treatment. Enthesitis was more frequent in patients with low disease activity by DAPSA score.
Psoriatic arthritis (PsA) is a chronic inflammatory skeletal and dermatological disease with heterogeneous clinical features and a strong relationship with the spondyloarthritis group, sharing several genetic, clinical, and radiographic characteristics [1] and with a prevalence in the western country populations around 0.07-0.42 [2]. Therapeutic options for both skin and joint diseases have dramatically improved, allowing efficient control of inflammatory activity in patients, including control of comorbidities such as metabolic and cardiovascular diseases (CVD) [3]. Inflammatory charge of psoriatic disease seems to be an independent risk factor for CVD in those patients with severe joint or skin disease [4], even in patients without traditional CVD risk factors and having a higher frequency of subclinical atherosclerosis than matched controls [5, 6].
PsA patients have multiple comorbidities such as obesity, hypertension, and hyperlipidemia [4, 7] and a higher prevalence of cardiovascular comorbidities compared to patients with psoriasis without PsA [8] and compared to the general population [9]. More than 50% of patients with PsA have at least one comorbidity and approximately 40% of patients can have three or more comorbidities [10, 11]. However, patients with PsA are at a higher risk of cardiovascular disease, including myocardial infarction and major adverse cardiovascular events (MACE) after accounting for traditional cardiovascular risk factors [12].
Obesity is a prevalent comorbidity in PsA, and this may be particularly important as adipose tissue plays a role in metabolism and immune-inflammatory processes affecting disease activity and response to therapy [13]. A higher body mass index (BMI) affects disease activity and response to therapy and has an impact on cardiovascular and metabolic morbidity [14]. It has been shown that metabolic syndrome (MetS) is associated with a state of chronic, low-grade inflammation [15] and Haroon et al [16] confirmed the high prevalence of MetS in patients with PsA compared to a control group probably reflecting the increasing burden of inflammation.
The Disease Activity Psoriatic Arthritis Index (DAPSA) is one of the main recommended targets for PsA treatment following EULAR recommendations, with a treat-to-target strategy [17]. Obese patients were found to have higher joint counts, C-reactive protein (CRP), Health Assessment Quality-Disability Index (HAQ-DI), and composite measures, including Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) [18]. Dietary intervention showed significant improvement in disease activity measures like DAS28-CRP, DAPSA, and HAQ-DI.
Therefore, we hypothesize that a higher body mass index and the presence metabolic syndrome are a risk factor for development much disease activity and worse response to therapy.
The aim of this study was to evaluate obesity and MetS among patients with PsA treated with synthetic disease-modifying antirheumatic drugs (csDMARD), naïve to biologics and its association with inflammatory activity status.
Study population
We performed a retrospective cross-sectional multicenter study of a cohort of patients with following inclusion criteria: ≥18 years of age, all patients with a diagnosis of PsA who met the CASPAR criteria [19], included in the “Sueiro Cohort” (20), treated with csDMARD without good response and waiting to start biologic treatment. As a control group, we used a previously described cohort of patients with PsA naïve to biologics and low disease activity or remission treated with csDMARD [21]. Key exclusion criteria were immune-mediated disease other than PsA, pregnancy, cancer or serious infection in the moment of evaluation.
All patients gave their informed consent to participate in the study, and the rules of good clinical practice (Helsinki declaration) were followed. The study was approved by the local clinical research ethics committee (reference no. 2015/671). Patient anonymity and confidentiality were preserved throughout the study.
Study design and variables
Patients were managed according to a standard protocol adopted at Rheumatology outpatient clinic of six hospitals and were followed up for at least 6 months. The study period spanned from 2017 to 2019.
Collected variables included age, sex, blood biochemistry, blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), HLA-B27, rheumatoid factor, glucocorticoid, NSAID and csDMARD, smoking habit, hyperuricemia, type 2 diabetes mellitus, obesity (BMI≥ 30 kg/m2), liver involvement (NAFLD, not including infectious or alcoholic liver disease) and the diagnosis of anxiety and depressive syndrome performed by the Health Mental Unit.
Metabolic syndrome (MetS) was defined as a combination of abdominal obesity, impaired fasting glucose, atherogenic dyslipidemia, and elevated blood pressure. Revised NCEP ATP III criteria [22] require at least three of the following components: abdominal obesity (waist circumference ≥90 cm for men, or ≥85 cm for women); triglycerides ≥150 mg/dL, and/or drug treatment for elevated triglycerides; high-density lipoprotein (HDL)-cholesterol <40>
Evaluation procedures for activity disease
The clinician´s criteria determined whether patients had a good response to DMARD. Disease activity status was supported by tender and swollen joint counts (TJC68 and SJC66) from patients before they started treatment with biologics. At the same time, patient-reported outcome measures were collected with Patient Global Assessment (PtGA 0-10 cm) and Patient Pain Assessment (Pain 0-10 cm). DAPSA and cDAPSA scores were calculated. Very low (VLDA), low (LDA), moderate (MoDA), and high disease activity (HDA) status were obtained by DAPSA and cDAPSA scores with their defined cut-offs elsewhere [23], when data were present in the records.
Statistical analysis
A descriptive statistical analysis of all the variables was performed, including central tendency and dispersion measures for continuous variables, and absolute and relative frequencies for categorical variables. The differences between quantitative variables with normal distribution according to the Kolmogorov–Smirnoff test were analyzed using Student’s t-test, or ANOVA test. Differences between quantitative non-normal variables were studied using non-parametric tests (Mann–Whitney U test or Kruskal–Wallis H test). Pearson’s chi-square or Fisher’s exact test was used for qualitative variables. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated using binary logistic regression analysis. Initially, univariate analysis was performed to examine the unadjusted associations of DAPSA and cDAPSA with its potential risk factors. The factors introduced in the univariate model were age, sex, disease duration, patterns of arthritis, nail involvement, dactylitis, enthesitis, use of NSAIDs, use of glucocorticoids, use of csDMARD, duration of systemic treatment, CVRF, and CRP. Significant variables in the univariate analysis (P<.10) were then introduced in a multivariate analysis with a backward stepwise approach. Tests were two-tailed with a significance level of 5%. Data were analyzed using SPSS version V21.0 statistical software (IBM Corp. NY, USA).
All patients: CVRF
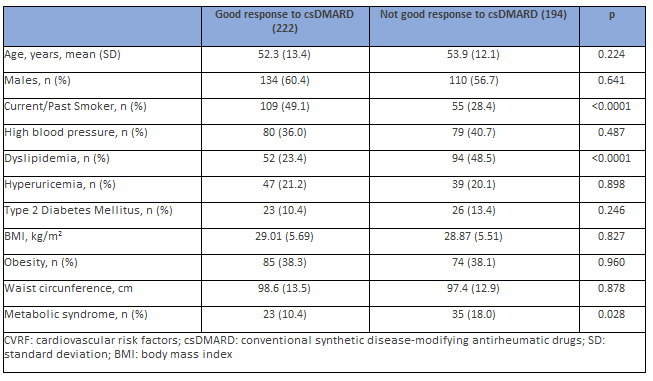
A total of 416 PsA patients were included in the study: 222 PsA patients kept on remission or low disease activity being treated without biologics (DAPSA score 8.3±4.5), and 194 who needed to be treated with bDMARD because they did not respond well to csDMARD. Both groups showed no differences with respect to age or sex. Dyslipidemia and MetS were more prevalent, and smoking habits (current/past) were less frequent in PsA patients who did not respond well to csDMARD (Table 1).
PsA patients who needed to be treated with bDMARD
Patients with a good response to csDMARD (in remission/LDA disease) were not included in the association analysis for inflammation because their clinical and biological activity indices were not elevated.
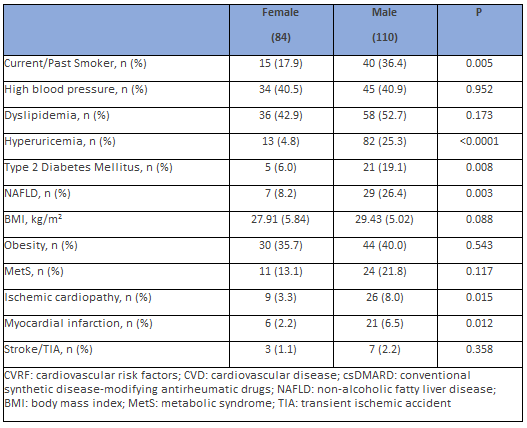
The frequency of traditional CVRF was more prevalent in men than in women: active smokers, diabetes mellitus, and hyperuricemia, but not hypertension, dyslipidemia, and obesity. NAFLD was also more frequent in men than in women. Women had less CVE than men (12 [4.4%] vs. 30 [9.2%], p = 0.021), but this difference was only in relation to angina and MI, but not in relation to stroke/TIA. Hyperuricemia (25.3% vs. 4.8%, p <0 xss=removed>
Patients with CVE had more nail psoriasis (41.7% vs. 20.8%, p=0.09), but there were no significant differences with regard enthesitis (p=0.562), dactylitis (p=0.780), or uveitis (p=0.553). Clinical patterns of PsA, treatment with NSAIDs, corticosteroids, or the positivity for HLA-B27 did not imply differences among genders.
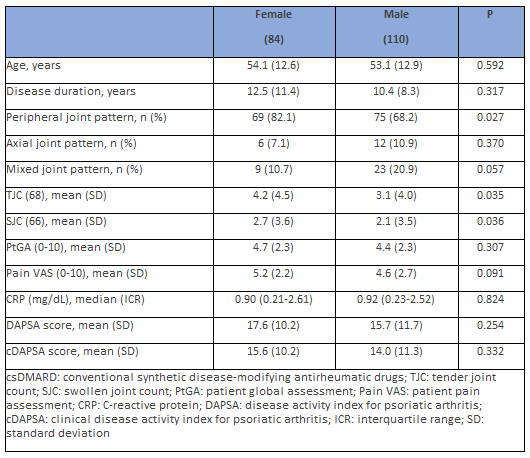
Most peripheral joint involvement was observed in women and axial affection in men (p = 0.027), but there were not significant differences between women and men in nail disease (17.1% vs. 25.4%), enthesitis (23.5% vs. 21.1%), dactylitis (12.7% vs. 12.9%), or uveitis (2.4% vs. 2.9%). Anxiety and depressive disorders were more prevalent in women (31% vs. 15.5%, p = 0.010).
Furthermore, women had joint counts much higher than men (TJC p =
0.035 and SJC p = 0.036), but there were no differences in the PtGA and levels of C-reactive protein. Patient pain VAS scores were higher in women but did not reach statistical significance. There was no difference between males and females with regard DAPSA or cDAPSA scores (Table 3), neither according to age (p = 0.622). The DAPSA and cDAPSA scores had a high positive correlation between both (rho = 0.972, p < 0>
A statistically significant difference was not observed between the DAPSA score and treatment with NSAIDs but was detected in relation to corticoids. The proportion of patients who received corticosteroids was significantly higher among patients with DAPSA>14 (28.8% vs. 11.5%; p = 0.006).
Metabolic syndrome and inflammatory activity
Patients with MetS were older than those without MetS, 59.6 (9.8) vs. 52.2 (13.1) years (p = 0.002). MetS was present in 18.0% of men and 13.1% of women (p = 0.117). MetS was not associated with clinical patterns (p = 0.782), serum levels of CRP (p = 0.681), DAPSA (p = 0.252), or cDAPSA score (p = 0.215). A higher frequency of enthesitis (p = 0.012) and lower of dactylitis (p 0.030) was observed.
In the linear logistic regression analysis (adjusted for age and sex), a high DAPSA score was not associated with MetS (p = 0.350). Binary regression analysis showed increased risk of MetS for age > 50 years old (OR 3.287 [95%CI: 1.258-8.591], p 0.015) and CRP > 0.5 mgr/dL (OR 2.684 [95%CI: 1.141-6.313], p 0.024) but not in relation to gender (OR 2.136 [95%CI: 0.932-4.893], p 0.073) neither to cDAPSA>13 (OR 1.539 [95%CI: 0.695-3.409], p 0.288).
Obesity and inflammatory activity
Patients with obesity were not significantly older than those without obesity (p = 0.106) and there were no differences in relation to sex (p = 0.543).
Obesity was not associated with clinical patterns (p = 0.322), onychopathy, or other clinical features. There was no observed correlation with frequency of enthesitis (p = 0.293) or dactylitis (p = 0.493). The intake of NSAIDs (33.6%) and corticosteroids (18.9%) implied no difference in relation to obesity (p = 0.666 and 0.371, respectively).
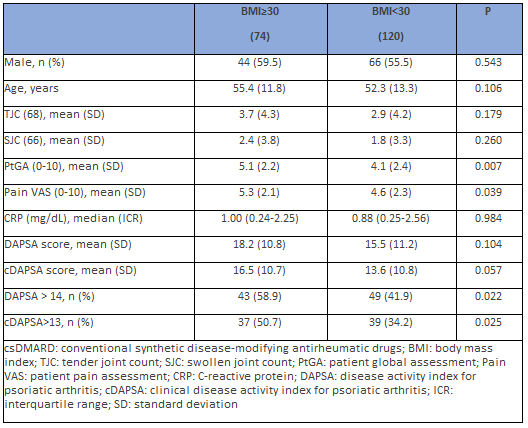
PtGA and pain VAS scores were higher in patients with obesity (p 0.007 and 0.044), but TJC, SJC, serum levels of CRP, DAPSA, or cDAPSA scores remained unchanged (Table 4). When the cut-off points of DAPSA were taken, patients with obesity had a higher frequency of DAPSA MoDA-HDA (p = 0.022) and the same was observed with cDAPSA (p = 0.025).
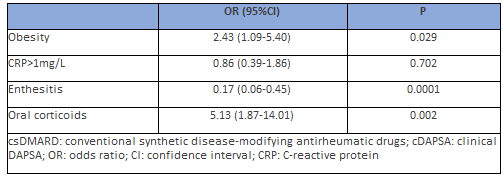
In the linear logistic regression analysis (adjusted for age and sex), a high DAPSA score was associated with obesity (p = 0.017) and CRP (p <0 xss=removed xss=removed> 50 years and sex) instead of DAPSA to include CRP as an independent variable, together with obesity, MetS, and other dichotomous variables. When it was taken “cDAPSA MoDA-HDA” as a dependent variable, it was observed that the presence of obesity and treatment with corticosteroids were independent factors for cDAPSA>13, and the presence of enthesitis for cDAPSA≤13 (Table 5).
Psoriatic arthritis is associated with increased cardiovascular comorbidity compared to control populations, including the risk of high blood pressure, dyslipidemia, diabetes mellitus, obesity, and metabolic syndrome, which results in increased cardiovascular events [8]. Likewise, several observational studies [24-26] have shown that the occurrence of cardiovascular events is directly associated with the severity of psoriasis, understanding the correlation between systemic inflammation and this increased risk. However, in a cohort study in which neither psoriasis nor severe psoriasis were associated with an increased risk of major cardiovascular events over a period of 3–5 years, after adjusting the parameters in relation to known cardiovascular disease risk factors [27], the risk of a major cardiovascular event was 36% higher in patients with psoriasis who also had inflammatory arthritis. Husted et al. [8] observed that the prevalence of hypertension, obesity, hyperlipidemia, type 2 diabetes mellitus, and at least one cardiovascular event in PsA patients was 37.1%, 30.0%, 20.7%, 12.0%, and 8.2%, respectively. This was significantly higher than in patients with psoriasis without arthritis, with unadjusted ORs ranging from 1.54 to 2.59. In multivariate analyses, hypertension remained significantly elevated (adjusted OR 2.17).
In our study, dyslipidemia and MetS were more prevalent in PsA patients who were going to start therapy with biologics when we compared them to patients with low charge of activity who were treated with csDMARDs, and with good response to them.
When we analyzed more in dept the most frequent CVRF, we found high percentages of hypertension, dyslipidemia, hyperuricemia, and diabetes among patients who experienced cardiovascular events, and these factors were directly related to male sex. The results obtained closely resemble those presented by Shah et al. [28], after analyzing the most frequent comorbidities associated with psoriatic arthritis in a cohort of US patients using real-life data. In this study, the authors observed that comorbidities in relation to the metabolic syndrome were higher in the population affected by this pathology than in the healthy population, with exception of obesity, which in the USA has a prevalence of 36.5%.
Given the strong link between PsA, systemic inflammation, metabolic syndrome and cardiovascular events, control of the inflammation associated with PsA may be applied beyond the skin and joint disease to prevent cardiovascular diseases. Limited data exist regarding the impact of csDMARD on cardiovascular outcomes. An association between methotrexate treatment and reduced cardiovascular risk has been found among patients with PsA using DMARDs who have been reported to have a lower cardiovascular risk than those who were not using them [4]. A meta-analysis of ten cohort studies including patients with rheumatoid arthritis, psoriasis, and PsA found that MTX therapy was associated with a 21% reduction in overall cardiovascular risk and 18% reduction in myocardial infarction risk [29].
The serum level of C-reactive protein is considered a marker of inflammation in several conditions, including psoriasis and rheumatoid arthritis, and high baseline levels of CRP have been found in some patients with psoriasis with or without PsA [30]. However, the clinical usefulness of C-reactive protein determination in cardiovascular disease in the general population has been questioned in relation to patients with pre-existing inflammatory conditions such as psoriasis [31]. In the present study, there were no differences between men and women or patients with or without CVD. Patients with obesity neither had higher levels of CRP when they were compared to no obese.
Recently, Gerdes et al. [32] suggested a neutral to favorable long‐term trend in metabolic and liver parameters under secukinumab treatment, and metabolic comorbidities were associated with increased hsCRP levels. In this exploratory post hoc analysis of pooled data from three phase 3
studies in patients with plaque psoriasis, psoriatic arthritis, metabolic syndrome, obesity, impaired glucose metabolism, and hyperuricemia, each were associated with increased hsCRP levels at baseline. Concomitant obesity attenuated the decline in hsCRP levels under treatment, which could reflect the role of systemic inflammatory processes in their pathophysiology.
The role of Th17-derived cytokines in the pathogenesis of obesity and related inflammatory diseases has been increasingly recognized [33]. Obesity has been shown to promote the expansion of IL-17-producing T cells in adipose tissue (especially visceral fat) and peripheral tissues [34, 35]. Accordingly, a significant increase in circulating IL-17 and IL-23 cytokines has also been observed in obese individuals compared with lean individuals in humans [36]. Supporting the implication of IL-17 in metabolic syndrome, the levels of IL-17R expression in the liver or muscle have been shown to correlate with insulin resistance [37], and IL-17 blocking results in a decrease in hepatic inflammation in non-alcoholic steatohepatitis syndrome [38].
Frequently, obese patients with PsA also have a higher disease severity. Mok et al. [39] observed that among 314 patients with PsA, obese patients tended to have a longer time to diagnosis compared to patients with a normal BMI, which leads to greater persistence over time of a systemic inflammatory state. The presence of arthritis may indicate an increased underlying systemic inflammation that may worsen comorbidities and cardiovascular outcomes. Obesity and its related metabolic abnormalities are more prevalent in patients with PsO and PsA than in those with other types of arthritis [39-41]. We could not observe any association between BMI>30 and tender or swollen joint counts but patients with BMI>35 (morbid obesity) had higher joint counts. Enthesitis was higher in obese patients, conversely to reported by Eder et al. [42]. We believe that patients with active enthesitis did not respond to csDMARD for this reason, requiring start treatment with bDMARD despite having a cDAPSA score in low activity, which is a consequence of not including an assessment of enthesitis in this score. Although systemic corticosteroids are not included in any guidelines, their prescription for PsA is still common in real life [43]. In the present study, patients with DAPSA>14 had a higher proportion of treatment with corticoids as a result a higher inflammatory activity. Patients using long-term low-dose prednisolone have hepatic insulin resistance and reduced peripheral nonoxidative glucose disposal indicating that low-dose prednisolone also exerts a deleterious effect on carbohydrate metabolism and abdominal adiposity [44].
In other reports [45-46], obese patients were found to have higher joint counts, C-reactive protein, Health Assessment Quality-Disability Index, and composite measures including cDAPSA. In our study, obesity was associated with higher DAPSA and cDAPSA scores, but the difference was not statistically significant. However, obese patients had a higher prevalence of DAPSA>14 (moderate-to-high activity) than patients without obesity. Both DAPSA and cDAPSA scores were had higher in patients with morbid obesity.
The study has some strengths and limitations. It was design as a cross-sectional study, and to evaluate the role of some specific comorbidities, such as cardiovascular, a longitudinal study could provide more data. It would be of interest to provide the MDA (minimal disease activity) status of our patients to evaluate disease activity status, including more domains of psoriatic disease than DAPSA score, like enthesitis or skin activity, since in other reports it has published those patients with a higher body mass index are less likely to achieve MDA and further studies are needed to answer these questions. The chronic inflammation in patients with high body mass index may be responsible for the increased risk for cardiovascular disease in PsA patients, and poor response to therapy.
Psoriatic arthritis has an increase in classic risk factors and cardiovascular events, especially in men and it also increases with age. There is abundant evidence of the association between chronic inflammation and cardiovascular risk factors, such as obesity or metabolic syndrome, but population studies are required to better understand the underlying mechanisms.
Some manifestations of PsA, such as enthesitis that are not included in the DAPSA score, have a significant inflammatory activity and must be considered when evaluating disease activity. Similarly, treatment with corticosteroids indicates that they have been established due to the inflammatory activity of PsA.
Early management of comorbidities, using the reference guidelines as well as a close control of disease activity, can contribute to the global improvement of these patients.
Take home messages:
The authors thank Mrs. Alba Pinto-Alonso for her grammatical support.
Conceptualization, JAPT, JMLV, CGP, FJMP and JAMM; Methodology, JAPT, JMLA, CIU, LFD, CGP, FJMP, JLGV and JAMM; validation, JAPT, JMLV, CGP, FJMP and JAMM; formal analysis, JAPT, JMLV, CGP, FJMP and JAMM; investigation, E.F., L.D., A.S., F.M., G.C., M.P. and F.P.; data curation, JAPT, JMLV, CGP, FJMP and JAMM; writing—original draft preparation, JAPT, JMLV and CGP; writing—review and editing, JAPT, JMLA, CIU, LFD, CGP, FJMP, JLGV and JAMM. All authors have read and agreed to the published version of the manuscript.
All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee (Ethical Committee of Santiago-Lugo, n. 2015/671) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all subjects involved in the study.
The data presented in this study are available upon request from the corresponding author. The data are not publicly available because of privacy restrictions.
None.
The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
