
Research Article | DOI: https://doi.org/10.31579/JNMIR.2020/001
*Corresponding Author: Biljana Ilkovska, Department of medical biochemistry, PHO Clinical Hospital dr. Trifun Panovski, Bitola, Macedonia.
Citation: Biljana Ilkovska, Bisera Kotevska, Sandra Hristovska, Petar Avramovski, Irena Kostovska, Katerina Tosheska-Trajkovska and Branimir Kanazirev, Laboratory Characteristics and Presentation of Multi-Organ Affection among Hospitalized Patients with SARS-CoV-2 Infection in Public Hospital in Bitola, J. New Medical Innovations and Research, 1(1): DOI: 10.31579/JNMIR.2020/001
Copyright: © 2020 Biljana Ilkovska. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 October 2020 | Accepted: 26 October 2020 | Published: 02 November 2020
Keywords: SARS – CoV 2; laboratory findings; multi organ failure;Leukocytosis;leucopenia;cardiac arrhythmias;aminotransferase;γ –glutamyl transferase;myocardial injury
Introduction: In December 2019, a highly infectious disease i.e. pneumonia caused by the coronavirus disease SARS-CoV-2, occurred in Wuhan, China, and the World Health Organization has declared its ongoing outbreak a pandemic. The clinical laboratory plays a key role in supporting the monitoring and management of SARS-CoV-2 disease.
Material and methods: Our study describes the laboratory characteristics of 103, SARS-CoV-2 patients hospitalized in the public hospital Trifun Panovski in the period April - June 2020. Only two patients died as a result of the SARS-CoV-2. The most common laboratory abnormalities were: elevated lactate dehydrogenase (LDH) and C-reactive protein (CRP).
Results: Leukocytosis was found in 23.3%, and leucopenia in 3% of patients with SARS – CoV-2. SARS-CoV-2 infection can be associated with myocardial injury, heart failure, vascular inflammation, myocarditis, cardiac arrhythmias, and hypoxic encephalopathy. We found increased values of alanine aminotransferase (ALT), aspartate aminotransferase (AST) and γ –glutamyl transferase (γ –GT) in 35 – 50% of patients. We detected affected renal function in 10% of our patients with SARS – CoV 2.
Conclusion:We identified potential biomarkers of disease severity. Our results provide guidance in risk assessment, clinical monitoring and therapy decision-making processes
In 2019 in China was registered first case in the world with SARS-CoV-2 viral pneumonia [1]. The geographical distribution of SARS-CoV-2 covers all continents except Antarctica. Epidemiologists in Wuhan believed the Huanan Seafood Wholesale Market in Wuhan is the point of origin of SARS-CoV-2, due to its connection to the trading of live wild animals [2]. At the time of writing, over 21,732,472 million confirmed SARS-CoV-2 cases and over 770,866 SARS-CoV-2 related deaths have been reported [3].
SARS-CoV-2 is highly contagious disease, with a basic reproduction number of between 1.4 and 6.5, and can be easily spread through coughs and sneezes, talking to infected persons, and touching the eyes, nose, or mouth after touching a contaminated surface [4].
The novel coronavirus belongs to lineage B of the genus beta coronavirus of the Coronavirus family, which includes SARS-CoV and MERS-CoV [5]. The SARS-CoV-2 is the seventh member of the coronavirus family that infects humans [6].
A recent study reported that fever, cough, myalgia or fatigue were common symptoms, and sputum production, headache, hemoptysis, and diarrhea were less common symptoms [7].
All patients had pneumonia and about half developed dyspnea [8]. Incubation duration of SARS-CoV-2 infection ranges from 2 to 14 days, and various studies demonstrate that symptoms are seen within an average of 4 to 7 days [9].
The SARS-CoV-2 clinical presentation can be: mild- the clinical symptoms were mild, and there was no or mild sign of pneumonia on imaging; moderate - showing fever and respiratory symptoms with radiological findings of pneumonia; severe- in accordance with any of the following: shortness of breath (RR ≥ 30 breaths/min); in resting state, oxygen saturation ≤ 93%; arterial partial pressure of oxygen/fraction of inspired oxygen ≦ 300 mmHg, cases with chest imaging showed obvious lesion progression more than 50% within 24–48 h; critical - one of the following: respiratory failure, requiring mechanical ventilation; septic shock; multiple organ failure.
Clinical laboratories are very important for management of SARS-CoV-2 disease. Hematological and biochemical parameters are important for detecting disease severity and monitoring SARS CoV 2 infection.
The aim of our study was to identify most laboratory biomarkers of disease severity.
This study was carried out from April to July 2020 at the Department of Medical Biochemistry and Department of infective diseases of Public Health Organization Clinical Hospital “D-r Trifun Panovski” in Bitola. Our study describes the laboratory characteristics of 103 SARS-CoV-2 infected patients hospitalized in Department of infective diseases with moderate stage of the diseases at the age of 17 to 86.
Ethics Committee of Health Organization Clinical hospital “d-r Trifun Panovski” approved the study, and all of the procedures were performed in accordance with ethical approval institutional guidelines. The study protocol followed the ethical guidelines of the most recent Declaration of Helsinki. Written consent was obtained from the participants prior to the start of the study.
Clinical and laboratory measurements - Patient respiratory samples, including nasopharyngeal swabs were collected and real-time polymerase chain reaction (RT-PCR) was used to confirm 2019-nCoV infection. Data includes: medical history, a physical examination, questionnaire information and laboratory findings of each patient. A confirmed case was defined by a positive result to RT-PCR of nasopharyngeal swab specimens. Blood samples were collected and drawn from an antecubital vein.
Complete blood count (CBC) was determined in ethylenediaminetetraacetic acid (K-EDTA) blood samples -using Sysmex XP 300/ Sysmex XS 1000 (Sysmex Co, Kobe, Japan) according to the manufacturer's instructions. The obtained indicators were as follows: white blood cell count (WBC x10⁹/L), neutrophil percentage (NEUT %), neutrophil count (NEUT(x10⁹/L), lymphocyte percentage (LYMPH %), lymphocyte count (LYMPH(x10⁹/L)), red blood cell count (RBC x10¹²/L), hemoglobin (HGB (g/l)), and platelets (PLT (x 10⁹ /L).
Biochemical analyses - Biochemical analyses were performed on Abbot Architect CI 4100 according to the manufacturer's instructions. We determined: alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBILI), direct bilirubin (DBILI), creatinine (CREA), urea (UR), γ-glutamyl transpeptidase (GGT), lactate dehydrogenase (LDH), creatin kinase (CK), creatin kinase MB fraction (CK-MB), glucose(GLUK), hypersensitive C-reactive protein (hsCRP) andiron.
The data are presented as mean± standard deviation (SD). The results were done with the SPSS version 13.
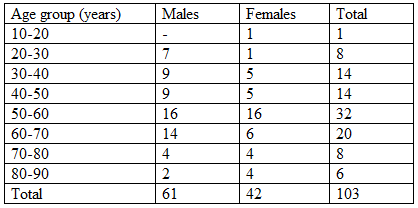
A total of 103 patients confirmed with SARS-CoV-2 infection were included in this study, of whom 61 (59.22%) were males and 42 (40.78%) were females. The median age was 53 years, the youngest patient was 17 years old and the oldest was 86 years of age. Study patients were divided in seven age groups presented in Table 1:
Hematological and biochemical features of COVID-19 patients are presented in Table 2 and Table 3.

The results are presented as: N (number), % (percent), Mean (min - max); WBC, white blood cells; Neut, neutrophils; Lymp, lymphocyte; RBC, red blood cells; HGB, hemoglobin; PLT, platelets.
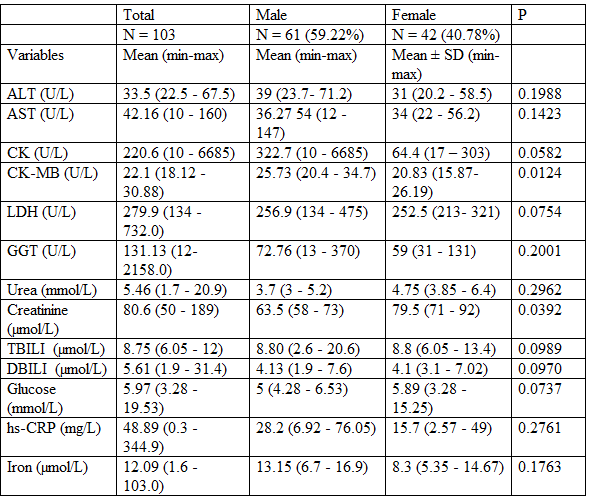
The results are presented as: N (number), % (percent), Mean (standard deviation) (min - max); Alanine aminotransferase (ALT), Aspartate aminotransferase (AST), Total bilirubin (TBILI), Direct bilirubin (DBILI), Creatinine (CREA), Urea (UR), γ-glutamyl transpeptidase (GGT), Lactate dehydrogenase (LDH), Creatin kinase (CK), Creatin kinase MB fraction (CK-MB), hypersensitive C-reactive protein (hsCRP).
Haematological parameters
Compared with the reference range our results showed that 24 SARS-CoV-2 infection positive patients (23.3%) had increased WBC levels (6 females and 18 males), 3 SARS-CoV-2 infection positive patients (2.9%) had decreased WBC count (2 females, 1 male) and 76 other patients had normal WBC count.
Compared with the reference range, 25 SARSCoV-2 infection positive patients (24.27%) had increased neutrophil levels (4 females and 21 males), 4 SARS-CoV-2 infection positive patients (3.8%) had decreased neutrophil levels (2 female, 2 males) and normal neutrophil levels were found in the 69 other patients.
Additionally, investigations revealed 19 patients with SARS-CoV-2 infection (18.4%) had increased lymphocytes (1 female and 18 males), 31 SARS-CoV-2 infection positive patients (30.1%) had lymphopenia (13 females and 18 males) and 53 other patients had normal lymphocyte levels.
Compared with the reference range, 25 SARS-CoV-2 infection positive patients (24.27%) had increased neutrophil levels, 4 SARS-CoV-2 infection positive patients (3.8%) had decreased neutrophil levels and 69 other patients had normal neutrophil levels.
Compared with the reference range, 3 SARS-CoV-2 infection positive patients (2.9%) had increased red blood cell count levels (3 males), 4 SARS-CoV-2 infection positive patients (3.8%) had decreased red blood cell count (1 female, 3 males) and normal red blood cell count levels were found in the 96 other patients.
Seven SARS-CoV-2 infection positive patients (6.8%) had increased hemoglobin levels (7 males), 19 SARS-CoV-2 infection positive patients (18.4%) had decreased hemoglobin concentration (11 females, 8 males) and normal hemoglobin levels were found in 77 other patients. Increased platelets levels were found in 25 SARS-CoV-2 infection positive patients (24.27%) (12 females and 13 males), 9 SARS-CoV-2 infection positive patients (8.7%) had decreased platelets (1 female, 8 males) and normal platelets count was found in the 69 other patients.
Biochemical tests:
Liver enzymes:
Activity of ALT was increased in 34 patients (10 females and 24 males), of AST in 46 patients (17 females and 29 males) and 26 patients (52%) had increased γ-glutamyl transpeptidase activity (10 females and 16 males). Over 66 patients had normal activity of ALT, 55 patients had normal values of AST and 28 patients had normal γ-glutamyl transpeptidase values.
Cardiac markers:
CK activity was increased in 13 patients (1 female and 12 males), 39 patients (11 females and 28 males) had increased activity for CK- MB fraction, 73 patients had normal CK values, and 48 patients had normal CK- MB fraction values.
Other biomarkers:
LDH
In laboratory practice was found that elevated LDH and CRP are the most frequent present in SARS CoV 2 infected patients. LDH activity was slightly elevated in 64 patients (26 females and 38 males), which represents 70% of examinee patients with SARS-CoV-2 infection. Only 27 SARS-CoV-2 positive patients had normal LDH values.
CRP
CRP was increased in 74 % of SARS-CoV-2 infection positive patients (27 females and 47 males). Twenty six patients had normal vales.
Kidney biomarkers:
Ten patients (4 women and 6 males) had increased values of urea and creatinine.
Iron
About iron homeostasis, 60% of examinee patients had decreased iron levels (11 females and 33 males) and 32 patients had normal values of iron.
The laboratory medicine is of crucial importance in diagnosis and treatment of COVID-19 patients. Routine hematological and biochemical tests are critical in process of diagnosis and management of COVID -19 patients. Inflammatory, hematological, cardiac, renal, hepatic and hematological markers can be used in process of assessment of severity status. Serum, plasma or whole blood specimens could be used for performance of different biochemical tests.
Our study was made in 103 patients with SARS CoV 2 infections who were hospitalized in our hospital in the period of April-June 2020.
Of total 103 admitted patients with SARS CoV2, two patients died. One patient was 47 years old male, hospitalized with chest pain, and increased cardiac markers. After initial treatment, all laboratory results were normalized, but on the 20th day of hospitalization, the virus has affected his kidneys and he died as a result of kidney damage. Second patient was 66 years old male, with previous liver damage, and after 10 days of proper medical treatment there was no improvement in his medical condition and he passed away.
Although respiratory symptoms dominate in the clinical picture in COVID-19, it is clear that virus can cause multiorgan failure.
Hematological findings implicate that lymphopaenia is a distinguishing characteristic of SARS – CoV-2 infection. Magnitude of lymphopaenia correlates with severity of disease. Lymphopenia was frequently detected on the hemogram (3%–83.2%) in studies of Lin [10] and Lippi [11].
In our study we found leukocytosis in 23.3%, leucopenia in 3%, lymphopenia was confirmed in 30% of patients with SARS – CoV-2. High neutrophil count is associated with poor outcomes and it may be result of secondary bacterial infection, On the other hand, low eosinophil count is commonly seen in patients with SARS – CoV-2 infection [12].
There was no significant change in hemoglobin levels of SARS-CoV-2 infection positive patients and healthy subjects in our study. Previous studies reported that patients with severe disease have significantly lower hemoglobin values compared with patients with mild conditions [13].
The liver appears to be the second organ involved, after the lungs. The cause of liver damage induced by SARS-CoV-2 is not fully understood, and the elevation of liver enzymes may result from cytokine storm or drug-induced liver damage. The SARS-CoV-2 infection is considered to be capable of infecting endothelial cells in the bile duct of the liver and causing inflammatory damage to the liver; the cellular damage in the liver may be the direct consequence of viral infection. Additionally, the virus may result in liver damage and testicular damage at varying levels [14].
SARS-CoV-2 infection is associated with mild elevation in ALT, AST and bilirubin. Elevated levels of AST, ALT and LDH has been firstly reported this year in 43% of the 99 SARS-CoV-2 cases from Wuhan [15].
We found increased ALT in 34%, AST in 46% and γ –glutamyl transferase in 52% of patients. Our results are in a correlation with study of Henry BM et al [16].
In addition, patients with abnormal liver tests had higher risks of progressing to severe disease [17].
Abnormal liver tests (AST, ALT, total bilirubin and γ –glutamyl transferase) were present in 76.3% of patients and 21.5% of respondents showed liver injury during hospitalization, in particular during the first two weeks after admittance [18].
Liver damage increases upon the prolongation of hospitalization, which could be associated with therapy protocols[19]. Patients on potential hepatotoxic therapies or previous liver damage should be monitored at least twice a week.
Recommendations of the IFCC task group is that monitoring of liver functional tests should be considered in hospital in patients with COVID-19.
Bilirubin increased by 5% associated with hepatocellular damage and cholestatic liver diseases could be seen SARS-CoV-2 patients. Hyperbilirubinemia was observed in studies of Guan, Lippi and Santoso [20-22].
LDH is a nonspecific marker of tissue damage. Many studies have shown elevated LDH activity, ranging from 27% to 76% [21, 22].
In our study, LDH was slightly elevated in 70% of examinee patients with SARS-CoV-2 infection. Only 27 SARS-CoV-2 positive patients had normal LDH values.
In the study of Chen et al. it was observed that advanced age, hypertension and high LDH levels at admission in the hospital were associated with the elevation in hospital mortality rates. LDH activitywas higher in severe cases than in mild and moderate cases [23].
SARS-CoV-2 infection affects cardiovascular system, too. SARS CoV2 infection is associated with myocardial injury, vascular inflammation, heart failure, myocarditis [17]. Underlying pathophysiology is not well understood but it can be a result of direct viral effect on a myocard, immune-mediated effect or as a result of respiratory failure or hypoxemia [24].
The authors suggested close monitoring of the cardiac functioning of all patients, especially the severe and critical ones, and to seek possible interventions for patients evincing features of abnormal cardiac injury.
Hence, it was concluded that heart injury signs arise in SARS-CoV-2, especially in older patients, hypertensives, and male patients with current smoking habits. Elevated levels of heart injury indicators are associated with higher mortality and shorter survival days [25].
Additionally, the discovery that SARS-CoV-2 patients had a simultaneous increase in α-hydroxybutyrate dehydrogenase, myoglobin, CK, or CK- MB fraction suggested that we should pay attention to patients with different degrees of skeletal muscle injuries.
The muscle-induced creatine kinase provides an insight, especially into the assessment of myocardial damage. Creatin kinase MB fraction was found to be high at 45%; higher rates were noted in patients with severe disease course [26].
Renal function was affected in 10% of Sars CoV2 positive patients. The kidneys are one of the most frequently affected extra-pulmonary organs in patients infected with SARS-CoV-2; especially, in those patients who are severely ill [8, 23, 27].
There are inconsistent results regarding the association of SARS – CoV-2 infection and acute kidney injury. Acute kidney injures are reported to vary from 1% to 42% [28]. Main causes of AKI can be: direct viral infection, haemo dynamic changes, thrombotic vascular processes, glomerular pathology or hypovolemia of kidneys.
Previous studies of patients affected by the 2013 SARS outbreak have shown that kidney damage is mainly characterized by tubular injury (as reflected by abnormal urine test results) and increased serum creatinine and urea nitrogen concentrations.
Although the underlying virologic mechanisms are not completely understood, it is plausible to speculate that there is binding of the virus to the ACE2 receptor, which is highly expressed in kidney tubules, causing glomerulopathy, acute tubular necrosis and protein leakage in the Bowman’s capsule [26].
Kennet found serum creatinine levels higher than 133 µmol/L amongst patients with severe SARS-CoV-2 [26].
In our study 60% of the patients had a decreased value of serum iron. Seventy four percents had an increased value of C-reactive protein. The high percentage of these indicators indicates the involvement of the immune response in patients, which correlates with previously published studies [29].
High levels of C-reactive protein were noted in the vast majority of SARS-CoV-2 patients (3%–91%) and shown to be associated with disease severity [21, 22].
C-reactive protein levels give an idea for disease severity and prognosis. Additionally, it is considered to be a potential early marker for sepsis and mortality. It is suggested that C-reactive protein level, especially at admission, may be critical for grading disease severity [30].
The prevention and control of the SARS-CoV-2 outbreak is well underway around the world and efforts must continue to target this virus.
This viral infection appears to adversely affect not only the respiratory system but also several other organ systems, including the urinary, liver, cardiovascular, gastrointestinal and neurological systems.
The Clinical Laboratory plays a key role in supporting the monitoring and management of SARS-CoV-2 disease
In the meantime, we believe that the front-line multidisciplinary team should carefully monitor multi-organ functions, which may also be the key to the survival of infected patients. We suggest an improved knowledge of SARS-CoV-2 related extra-pulmonary complications will help to develop better medical management strategies for these patients.
We suggest that CBC should be performed in each patient with COVID-19 infection, because lymphopenia is a hallmark in symptomatic patients and elevated neutrophil to lymphocyte ratio is associated with bad clinical outcomes. We recommend CRP or erythrocyte sedimentation rate (ERS) to be monitored in COVID-19 patient because their increased levels are associated with worse clinical outcomes.
Increased levels of AST, ALT and bilirubin, LDH, Urea and creatinine are associated with poor prognosis. Albumin levels should be monitored because they reflects an acute inflammatory state or synthetic liver dysfunctions.
Biochemical and hematological tests are very important for clinical monitoring and therapy protocol for the patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
