
Research Article | DOI: https://doi.org/10.31579/2690-4861/570
1 Doctor of Medical Sciences (MD), Professor, Academic Secretary, A.V. Vishnevsky National Medical Research Center of Surgery, Moscow, Russia.
2 Researcher of Ultrasound Diagnostics Department, A.V. Vishnevsky National Medical Research Center of Surgery, Moscow, Russia.
3 Candidate of medical sciences (PhD), Head of Ultrasound Diagnostics Department, A.V. Vishnevsky National Medical Research Center of Surgery, Moscow, Russia.
4 postgraduate student of Endovascular Surgery Center, A.V. Vishnevsky National Medical Research Center of Surgery, Moscow, Russia.
5 Candidate of Medical Sciences (PhD), Senior Researcher of Radiology Department, A.V. Vishnevsky National Medical Research Center of Surgery, Moscow, Russia.
6 Doctor of Medical Sciences (MD), Head of Urology Department, A.V. Vishnevsky National Medical Research Center of Surgery, Moscow, Russia.
*Corresponding Author: Stepanova Yulia Aleksandrovna, Doctor of Medical Sciences (MD), Professor, Academic Secretary, A.V. Vishnevsky National Medical Research Center of Surgery, Moscow, Russia.
Citation: Stepanova Yu.A., Raguzina V.Yu., Kadyrova M., Galstyan A.V., Kondratiev E.V.,et al, (2024), Kidney Cancer with Concomitant/Competing Surgical Diseases: Multidisciplinary Approach to Examination and Treatment, International Journal of Clinical Case Reports and Reviews, 20(3); DOI:10.31579/2690-4861/570
Copyright: © 2024, Stepanova Yulia Aleksandrovna. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 October 2024 | Accepted: 21 October 2024 | Published: 05 December 2024
Keywords: kidney cancer; concomitant/competing surgical diseases; cardiovascular diseases; primary multiple cancer; benign surgical diseases; diagnosis; staged treatment
Purpose: to develop a program of complex instrumental diagnostics based on the data of kidney cancer patients with concomitant/competing surgical diseases accumulated at A.V. Vishnevsky NMRC of Surgery, evaluate and analyze the results of a comprehensive examination and treatment of these patients.
Materials and methods: Results of diagnostics and surgical treatment of 26 kidney cancer patients with concomitant/competing surgical diseases (males - 84.6%, average age 61.1 years (38-82 years).
Results: A possible combination of surgical pathologies made it necessary to develop a comprehensive program for examining patients, aimed at identifying all possible pathological changes in human organs/systems. This program is possible and works effectively only in a multidisciplinary hospital.
Identified concomitant/competing surgical pathologies can be divided into three groups:
Group I - cardiovascular diseases (14 (53.8%): critical stenosis of the coronary arteries (10); aortic aneurysm (1); external iliac artery and vein arteriovenous fistulas (1); cardiac arrhythmias (2) (the total number of patients is higher, because of one patient had coronary artery stenosis in combination with arrhythmia).
Group II - malignant tumors of other localization (9 (34.6%): lung cancer (1); esophageal cancer (1); stomach cancer (3); neuroendocrine and hepatocellular liver cancer - 1 case each; colon cancer (1); prostate cancer (1).
Group III - benign surgical diseases (4 (15.4%): choledocholithiasis (1); choledochal stricture (1); inguinal hernia (1); spleen hemangioma (1).
The total number of patients in all three groups is larger because one patient had synchronous kidney and stomach cancer and coronary artery stenosis.
Further, a personal consultation was held for each patient with the definition of treatment tactics: surgical correction of pathological changes that had a more significant threat to life (cardiovascular diseases more often) was performed first of all.
Conclusion: The developed system for examining patients who come to the surgical hospital for kidney cancer allows timely identification and elimination of life-threatening pathological conditions and, thus, improving the results of patients with this pathology treatment, which is possible only in a multidisciplinary surgical hospital when working with a multidisciplinary team.
Kidney cancer accounts for about 5% of cancer incidence among men and 3% among women. The most common variant of kidney cancer is clear cell carcinoma, which accounts for about 70-85% of detected cases [1].
Every year, 403.3 thousand new cases of kidney cancer are registered in the world (2.0% of all malignant neoplasms, rank 15) and 175.1 thousand deaths from this pathology (2.0% of all deaths) in Russia for the period from 2012 to 2017 standardized incidence rates increased by 13.8% in men (from 12.3 to 14.0 per 100,000 population, world standard) and by 16.4% in women (from 6.7 to 7.8 per 100,000 population). The increase in the incidence of kidney cancer is due, among other things, to the improvement of early diagnosis [2].
The average age of patients diagnosed with a malignant neoplasm of the kidney for the first time in their lives is 61.8 years [3]. Therefore, often, by this age, patients also have other pathological, often neglected, changes that require surgical treatment. Multimorbidity in the elderly has become the rule rather than the exception today. Most often, these are cardiovascular diseases (CVD) and primary multiple tumors.
With aging, the function of organs and systems of the human body declines including the immune system resulting in a diminished response to various pathogens and a chronic inflammatory process; these changes, in addition to other risk factors, contribute to the development of multiple morbid conditions including CVD and cancer. Multimorbidity in the elderly has become the rule rather than the exception today. Further, this association between CVD and cancer, at least partially, is explained by both diseases sharing common risk factors and from accelerated vascular aging due to cancer and its associated therapies. Multiple studies have shown that the incidence of cancer is much higher in patients with CVD compared to the general population [4].
CVD is currently the leading cause of death and disability worldwide. These diseases are caused by atherosclerotic lesions of the main arteries and are still one of the main causes of death and disability in the population worldwide [5].
It is also possible and the development of primary multiple cancer. Multiple primary tumors (MPT) are the independent occurrence and development of two or more neoplasms in one patient [6, 7]. The development in one organism of two, three, and sometimes more malignant tumors indicates the individual characteristics of the patient or the specific influences on the organism of its habitat. In recent years, there has been an increase in the frequency of multiple neoplasms. The factors influencing the increase in the incidence of malignant MPT are: an increase in the average life expectancy, both in general and after successful treatment of oncological diseases; increase in the intensity of carcinogenic effects, urbanization, accumulation of hereditary burden, improvement in the diagnosis of oncological diseases. One of the leading roles in the development of malignant MPT is played by a decrease in the immune status [8].
It is also possible to combine kidney cancer with other benign surgical diseases, such as chronic calculous cholecystitis, hernia, and others [9-11].
Since 2012 at Oncourology Department of A.V. Vishnevsky NMRC of Surgery about 70 patients with kidney cancer are operated on annually. Considering the average age of patients at which kidney cancer is detected, often these patients were simultaneously diagnosed with other diseases requiring surgical treatment (combined/competing). After a retrospective analysis of the data of patients who applied for and underwent surgical treatment for kidney cancer, it was found that about 8.0% of patients who had various competing surgical diseases left the Center for further examination and did not return for surgical treatment of kidney cancer. Thus, a possible combination of surgical pathologies made it necessary to develop a comprehensive program for examining patients aimed at identifying all possible pathological changes in human organs and systems in order to make a complete comprehensive diagnosis and determine the stages of treatment.
Purpose
to develop a program of complex instrumental diagnostics based on the patients with kidney cancer examination data at A.V. Vishnevsky NMRC of Surgery, evaluate and analyze the results of a comprehensive examination and treatment of patients with kidney cancer with combined/competing surgical diseases.
The experience in diagnosing and treating of 26 patients with kidney cancer and combined surgical diseases accumulated at A.V. Vishnevsky NMRC of Surgery (males predominated - 22 (84.6%), the average age was 61.1 years (38-82 years).
An analysis of data on comorbidities in patients with kidney cancer showed that when preparing a patient for surgery in a multidisciplinary surgical hospital, and if patients have complaints and / or anamnestic data on diseases of the cardiovascular system, digestive tract or other organ systems, it is advisable carrying out the following studies:
• echocardiography;
• ultrasound of the vessels of the lower extremities and brachycephalic arteries;
• coronary angiography;
• with controversial results of coronary angiography - scintigraphy and stress tests;
• in the presence of heart rhythm pathology - Holter monitoring;
• esophagogastroduodenoscopy;
• ultrasound of the abdominal cavity and retroperitoneal space, if necessary, additional examination - MSCT / MRI with or without contrast enhancement;
• in the presence of diabetes - ultrasound of the thyroid gland.
26 patients had associated/competing surgical diseases in our study. Based on the data of the preoperative examination, the patients were divided into three groups depending on the comorbidity:
1. Group I - CVD (n = 14 (53.8%);
2. Group II - malignant tumors of other localization (thoracic, abdominal and pelvic (n = 9 (34.6%);
3. III group - abdominal organs benign surgical diseases (n = 4 (15.4%).
The total number of patients in all three groups is larger because one patient had synchronous kidney and stomach cancer and coronary artery stenosis.
The diseases of each groups are presented in Table 1.
| Group I, n = 14 (53.8%) |
• critical stenosis of the coronary arteries - 11 • aortic aneurysm - 1 • external iliac arteriovenous fistulas - 1 • ventricular extrasystole – 2 *one patient had coronary artery stenosis in combination with arrhythmia |
| Group II, n = 9 (34.6%) |
• lung cancer - 1 • cancer of the esophagus - 1 • stomach cancer - 2 • neuroendocrine liver cancer – 1 • hepatocellular cancer – 1 • colon cancer - 1 • prostate cancer - 1 |
| Group III, n = 4 (15.4%) |
• calculous cholecystitis, choledocholithiasis - 1 • choledochal stricture - 1 • inguinal hernia - 1 • spleen hemangioma - 1 |
Table 1: List of concomitant/competing surgical diseases in patients with diagnosed kidney cancer, assigned to different groups
In addition, in patients with kidney cancer, intraluminal thrombosis of various levels was also detected in 9 (34.6%) cases, and metastasis in the lung was also simultaneously detected in 1 case.
Further, a personal consultation was held for each patient with the definition of treatment tactics: first of all, surgical correction of pathological changes that had a more significant threat to life was performed (CVD were more often).
The results of patients treatment’s by groups.
First group
In the presence of kidney cancer and CVD, the surgical treatment presented in Table 2 was performed.
| Pathology | Stages of surgical treatment |
| coronary arteries critical stenosis - 11 | • first stage - both open and endovascular interventions - 9 cases; • second stage - endovascular interventions - 2 cases (kidney cancer with the inferior vena cava thrombus) |
| aortic aneurysm – 1 | • first stage - resection of the infrarenal aorta aneurysm with aorto-bifemoral prosthesis - 1 |
| external iliac arterio-venous fistulas – 1 | • simultaneous intervention - 1 |
| ventricular extrasystole – 2 | • first stage - coronary artery bypass grafting with RFA modification of the Cox-Maze operation – 1 case • second stage - endovascular intervention - 1 case (kidney cancer with inferior vena cava thrombus) |
Table 2: Stages of surgical treatment of patients in group I
In order to illustrate the examination and treatment of patients in group I, clinical case 1 is presented.
Man D., aged 75, complained of aching pain in the right lumbar region, severe hematuria, general weakness.
Examination: ultrasound - hypervascular tumor of the right kidney, tumor thrombus in the renal and inferior vena cava (Mayo III) (Fig. 1); MSCT - tumor of the right kidney, tumor thrombus in the inferior vena cava (Fig. 2); coronary angiography - critical stenosis of the coronary arteries (stenosis of the anterior interventricular branch (AIB) in the middle third up to 85-90%) (Fig. 3).
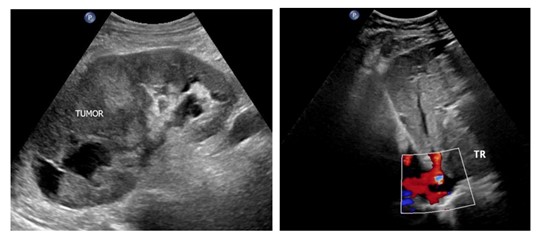
Figure 1: Ultrasound: a – kidney tumor (TUMOR); b - inferior vena cava tumor thrombus (TR)

Figure 2: MSCT, right kidney tumor with the inferior vena cava thrombus
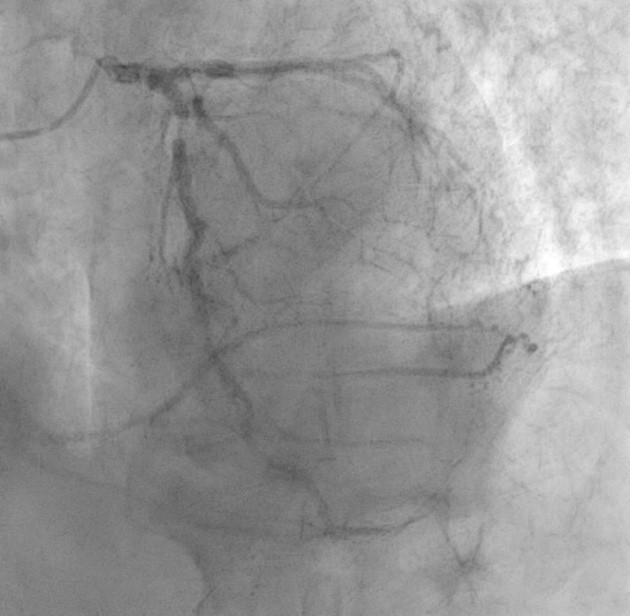
Figure 3: Coronarogram, LAD stenosis in the middle third up to 85-90% (arrow)
Based on the results of the medical consultation, it was decided to perform aorto- and mammary-coronary bypass grafting at the first stage (Fig. 4) and right nephrectomy with inferior vena cava thrombectomy from at the second stage (Figure. 5).
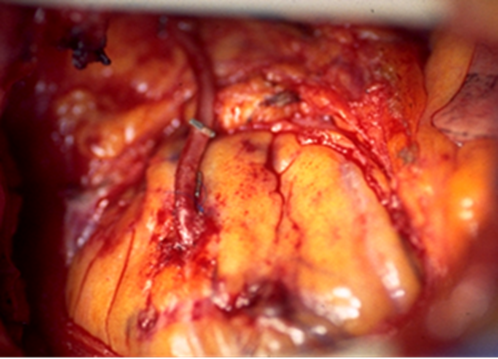
Figure 4: Intraoperative photo, autovenous coronary artery bypass grafting

Figure 5: Removed kidney with tumor thrombus
The total time of examination and treatment of patients group I (including surgical treatment of both pathologies) varied from 16 to 266 days, on average – 113.2±89.5, median – 87,5 (51.0-155.0).
Second group.
In the presence of kidney cancer and a malignant tumor of another localization (organs of the chest, abdominal cavity and small pelvis), the surgical treatment presented in Table 3 was performed.
| Pathology | Stages of surgical treatment |
| lung cancer - 1 (with mts in the same lung) | first stage - kidney surgery, second stage - lung resection |
esophageal cancer – 1 | first stage - esophagus resection with plastic, second stage - kidney surgery |
| stomach cancer - 3 | • first stage - endovascular interventions - 1 cases, second stage - simultaneous stomach and kidney surgery; • simultaneous surgery |
| neuroendocrine liver cancer - 1 | simultaneous surgery |
| hepatocellular cancer - 1 | first stage - hemyhepatectomy, second stage - kidney surgery |
| colon cancer - 1 | simultaneous robot-assisted surgery |
| prostate cancer - 1 | first stage – prostatectomy, second stage - kidney surgery |
Table 3: Stages of surgical treatment of patients in group II
In order to illustrate the examination and treatment of patients in group II, clinical case 2 is presented.
Man S., aged 65. The left kidney lesion was diagnosed during a routine ultrasound at the place of residence. He turned to the Urology Department of our Center for additional examination and determination of further tactics.
Examination: MSCT - left kidney two tumors, segmental renal vein tumor thrombosis (Fig. 5); gastroscopy - an ulcer of the stomach cardial part (biopsy: fragments of adenocarcinoma of a tubular and cribriform structure with superficial foci) (Figure 6).
Based on the results of the medical consultation, it was decided to perform a simultaneous operation. First, a laparoscopic resection of the left kidney was performed (Figure 7), then an extended combined proximal subtotal stomach resection, interposition of jejunum segment of the type of jejunogastroplasty.
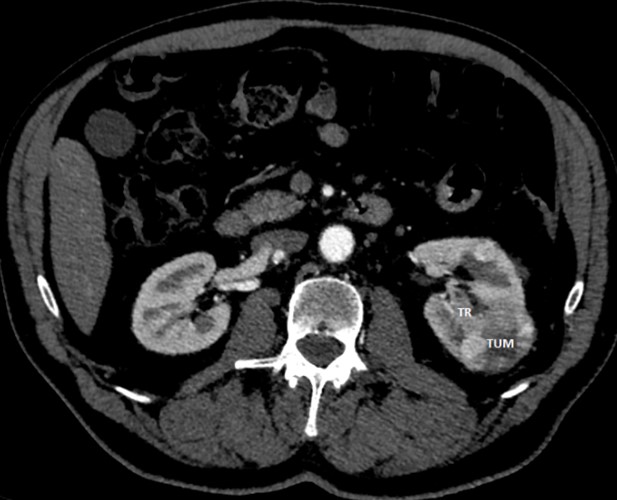
Figure 6: MSCT, left kidney cancer (TUM) with segmental renal vein tumor thrombus (TR)
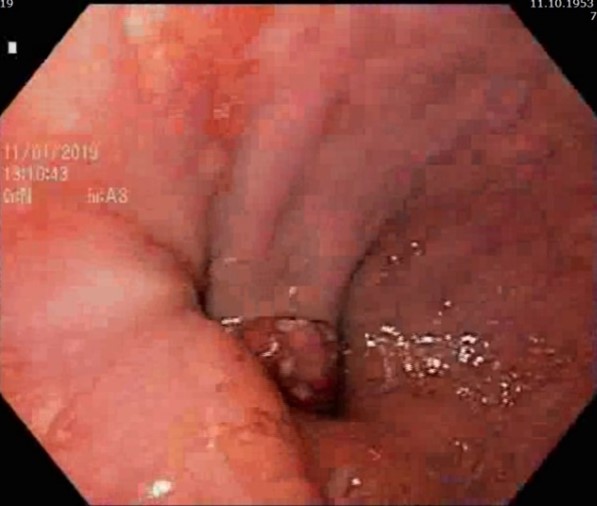
Figure 7: Cardioesophageal junction C-r
The total time of examination and treatment of patients group II (including surgical treatment of both pathologies) varied 10 to 89 days, on average – 44.0±26.3, median – 49.0 (25.5-54.5).
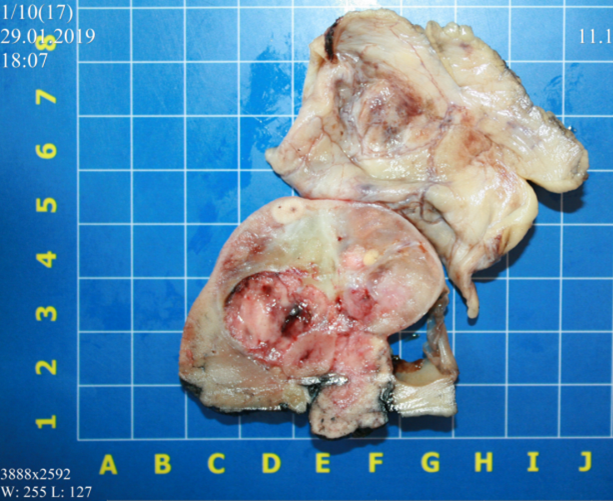
Figure 8: Sectional of the resected kidney
Third group.
In the presence of kidney cancer and benign surgical disease of the abdominal organs, the surgical treatment presented in Table 4 was performed.
| Pathology | Stages of surgical treatment |
| calculous cholecystitis, choledocholithiasis - 1 | first stage - cholecystectomy and lithoextraction, second stage - kidney surgery |
| choledochal stricture - 1 | first stage - choledochus stenting, second stage - kidney surgery |
| inguinal hernia - 1 | first stage - kidney surgery, second stage - hernia repair |
| spleen hemangioma - 1 | first stage - kidney surgery, hemangioma - dynamic observation |
Table 4: Stages of surgical treatment of patients in group III
In order to illustrate the examination and treatment of patients in group III, clinical case 3 is presented.
Woman R., aged 65, after an attack of biliary colic, yellowing of the skin and sclera, routinely sought medical help.
According to ultrasound at the place of residence: signs of exacerbation of chronic calculous cholecystitis, expansion of intra- and extrahepatic bile ducts were detected.
He turned to our Center for additional examination and determination of further tactics.
Examination: gastroscopy - an expansion of the longitudinal fold up to 10 mm (wedged calculus?), no bile from the mouth is noted. An additional examination was prescribed within the framework of MR cholangiography: calculous cholecystitis, choledocholithiasis (Fig. 8), signs of liver fatty degeneration; right kidney solid-cystic lesion, right kidney staghorn calculus. Ultrasound: right kidney hypovascular solid-cystic tumor in the middle segment is detected (Figure. 9), large staghorn calculus 45 mm in size in the right kidney sinus, with a wide acoustic shadow is detected.
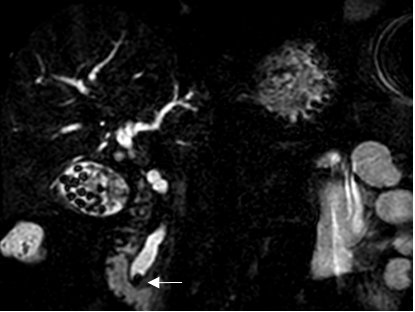
Figure 9: MRI, calculous cholecystitis, choledocholethiasis, biliary hypertension, calculus in the lumen of the intrapancreatic choledochus (arrow)
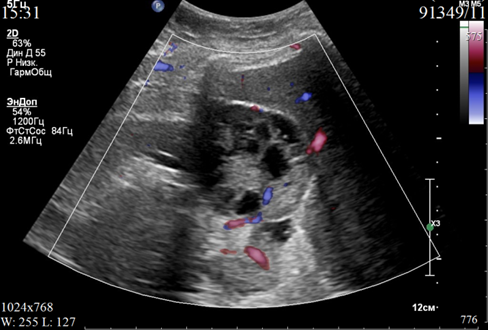
Figure 10: Ultrasound, solid-cystic hypovascular kidney tumor
Based on the results of the medical consultation, it was decided to perform the first stage of cholecystectomy and lithoextraction, the second - resection of the right kidney.
The total time of examination and treatment of patients group III (including surgical treatment of both pathologies) varied from 14 to 78 days, on average – 46.75±33.94, median – 47,5 (17.5-76.0).
Thus, the data obtained indicate that the above approach to the diagnosis and staged treatment of kidney cancer with concomitant/competing surgical pathologies within one hospital allows to reduce the total time of treatment of patients (on average – 77.48±72.15 days, median – 55.0 (23.0-89.0). An important factor is the patient constant contact with the attending physician who control the situation at all stages, which significantly positively affects the emotional state of such a complex category of patients.
A possible combination of surgical pathologies made it necessary to develop a comprehensive program for examining patients aimed at identifying all possible pathological changes in human organs and systems. Simultaneous operations, as well as operations performed within the same hospitalization, not only have high economic efficiency, but also make it possible to exclude repeated hospitalizations and anesthesia for the patient, reduce the total period of treatment for patients with two or more diseases, compared with multi-stage treatment. This program of examination and treatment is possible and works effectively only in a multidisciplinary hospital.
Multidisciplinary teamwork has been introduced into cancer care systems in many European countries, USA and Australia, without any clear evidence of its effectiveness.
Conducting regular patient discussions with a multidisciplinary team of specialists requires significant time and financial costs. Therefore, it is important to evaluate the empirical benefits of such a practice. Of course, it is clear that multidisciplinary discussions influence the practice of assessing the condition of patients and the tactics of their management. Over the past 10 years, the appropriateness of such an approach has been actively discussed in the literature. However, most of these are, after all, systematic reviews of the literature [12-15]. Although there are attempts to analyze the effectiveness of a multidisciplinary team when discussing patients with an analysis of their own data and even an assessment of the financial benefits of such an approach [16-18].
In our study, we attempted to analyze possible comorbid conditions in patients with kidney cancer. These are, first of all, CVD, which, in our
opinion, work here in the same way as with cancer of other organs: with age, the functions of the organs and systems of the human body decrease, including the immune system, which leads to a chronic inflammatory process, oxidative stress, endothelial dysfunction and, as a consequence, the development of the oncological process. Next, this is primary multiple cancer, which, as is already clear, we will encounter more and more often. However, we should also take into account the possibility of developing benign surgical diseases, such as chronic calculous cholecystitis, its complications and variants of postoperative manifestations, hernias, benign lesions. According to modern epidemiology, chronic cholecystitis affects 17 to 20% of the adult population of the planet [19], so the probability of its comorbidity with other diseases is high and this should be taken into account when assessing the condition of a patient with another disease. For example, Reimar W. Thomsen et al. in 2008 conducted a cohort study of 51,228 patients with cancer identified in medical databases of western Denmark between 1995 and 2003. Cholecystitis was more common in cancer patients than in the general population, especially during the first 6 months after cancer diagnosis. [9].
Overall, research on the effectiveness of a multidisciplinary approach to patient assessment is currently highly relevant. This is especially true for patients with cancer. About half of people with cancer experience personal economic hardship related to the disease and its treatment, a problem known as financial toxicity [20]. Most of the published studies are either reviews or poorly analyzed from the point of view of evidence-based medicine. And it is a set of large groups combining oncological and general somatic diseases and cross-analysis of data on these groups that will allow us to develop the most effective and cost-effective approach to making the most complete diagnosis and developing the most effective treatment tactics for such patients.
As the aging population increases, CVD, cancer, and multimorbidity will continue to constitute a major health problem in the years to come. The physician who is taking care of such a patient, in addition to knowledge, requires clinical wisdom, clinical experience, and common sense in order to apply the continuous evolving knowledge to the individual patient.
The developed system for examining patients who come to the surgical hospital for kidney cancer makes it possible to identify and eliminate life-threatening pathological conditions in time (both simultaneously and in stages) and, thus, improve the results of treatment of patients with this pathology, which is possible only in a multidisciplinary surgical hospital when working with a multidisciplinary team.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
