
Research Article | DOI: https://doi.org/10.31579/2641-0419/032
On behalf of the Korea Acute Myocardial Infarction Registry - National Institute of Health (KAMIR-NIH) Investigators 1Division of Cardiology, Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University, School of Medicine, Daejeon, Korea
2Chonnam National University Hospital, Chonnam National University, School of Medicine, Gwangju, Republic of Korea 3Kyungpook National University Hospital, Kyungpook National University, School of Medicine, Daegu, Republic of Korea 4Yeungnam University Hospital, Daegu, Republic of Korea
5Kyunghee University College of Medicine, Seoul, Republic of Korea
6Seoul National University Hospital, Seoul National University, School of Medicine, Seoul, Republic of Korea
7Chungbuk National University Hospital, Chungbuk National University, School of Medicine, Cheongju, Republic of Korea 8Samsung Medical Center, Sungkyunkwan University, School of Medicine, Seoul, Republic of Korea
*Corresponding Author: N, Division of Cardiology, Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University, School of Medicine, Daejeon, Korea
Citation: Kye T. Ahn., Seok-Woo Seong., Kim M., Jin-Ok Jeong., Seon-Ah Jin. et al. (2020) Impact of thrombus aspiration one-year cardiac mortality during primary PCI in STEMI patients with total occlusion; from Korea Acute Myocardial Infarction Registry National Institute of Health. J Clinical Cardiology and Cardiovascular Interventions, 3(3); DOI:10.31579/2641-0419/032
Copyright: © 2020 Seok-Woo Seong. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 November 2019 | Accepted: 27 January 2020 | Published: 04 February 2020
Keywords: thrombus aspiration; myocardial infarction; percutaneous coronary intervention
Background: The clinical impact of intracoronary thrombus aspiration (TA) during primary percutaneous coronary intervention (PCI) in patients with ST-segment elevation myocardial infarction (STEMI) is unclear. We investigated to evaluate whether TA during primary PCI reduces one-year mortality.
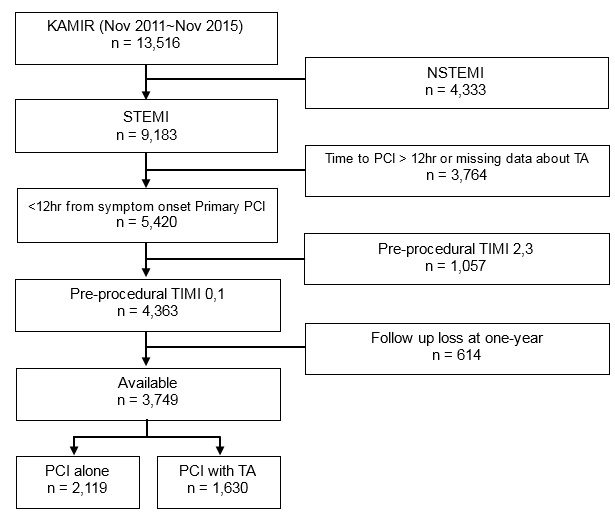
Methods: From the Korea Acute Myocardial Infarction Registry-National Institute of Health, 3749 patients with STEMI who were undergoing primary PCI within 12 hours (60.8±12.9 years, 18.7% women) and shown pre-procedural Thrombolysis In Myocardial Infarction (TIMI) flow 0, 1 in coronary angiography were enrolled between November 2011 and November 2015 during one-year follow up. The patients were divided into two groups according to TA during primary PCI: PCI with TA (n=1630) and PCI alone (n=2119). The primary end-point was major adverse cardiac events (MACE), defined as the composite of cardiovascular death (CVD), stroke or recurrent MI at one-year. The secondary efficacy end-point were all-cause of mortality and CVD at one-year.
Results: PCI with TA did not reduce the risk of MACE (OR: 0.598, 95% CI: 0.737-1.160, p=0.499), all-cause mortality (OR: 0.898, 95% CI: 0.705-1.144, p=0.383) and CVD (OR: 0.893, 95% CI: 0.683-1.168, p=0.408) in all patients during one-year follow up. The trend did not change after propensity score matching. In subgroup analysis, there was no efficacy of clinical outcome during one-year follow up.
Conclusions: Primary PCI with TA did not reduce MACE and all-cause mortality among patients with STEMI and pre-procedural TIMI flow 0,1 during one-year follow up.
Manual thrombus aspiration (TA) during primary percutaneous coronary intervention (PCI) reduces thrombus burden and improves markers of myocardial reperfusion in patients with acute ST-elevation myocardial infarction (STEMI) [1,2]. However, its clinical benefit has been a contentious point of debate. The Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS) trial [3] and other several studies [4-6] showed a mortality reduction with TA. In contrast, 2 recent multi-center randomized trials, the Trial of Routine Aspiration Thrombectomy with PCI versus PCI Alone in Patients with STEMI (TOTAL) [7] and the Thrombus Aspiration in ST-Elevation myocardial infarction in Scandinavia (TASTE) [8,9] failed to show a significant reduction in clinical events including mortality.
There remain unanswered questions on the efficacy of PCI with TA including whether PCI with TA truly is of clinical benefit and which subgroups may or may not benefit from the procedure. In the present study, we sought to evaluate clinical impact of TA during primary PCI in STEMI patients with pre-procedural Thrombolysis In Myocardial Infarction (TIMI) flow 0, 1
2. Materials and Methods
2.1 Study design and population
The study population was derived from the Korea Acute Myocardial Infarction Registry-National Institutes of Health (KAMIR-NIH) between November 2011 and November 2015. The KAMIR-NIH is a prospective, multicenter, web-based observational cohort study to develop the prognostic and surveillance index of Korean patients with acute myocardial infarction (AMI) from 20 centers in Korea and has been performed to support by a grant of Korea Centers for Disease Control and Prevention since November 2011. Trained study coordinators at each participating institution collected the data using a standardized format. Standardized definitions of all variables were determined by the steering committee board of KAMIR-NIH.
We analyzed a total of 13516 patients with AMI undergoing primary PCI.
Inclusion criteria for the current study are as follows
We therefore enrolled a total of patients in the current study. The study flow diagram is shown in Figure. 1. The current study was approved by the Institutional Review Board (IRB) of our medical institution. All patients proved written, informed consent for participant in the registry.
The primary efficacy end-point was one-year major adverse cardiac events (MACE), defined as the cardiovascular death (CVD), myocardial infarction (MI) or stroke. one-year all cause of mortality. The secondary efficacy end-points were one-year all cause of mortality and CVD. The incidence of “definite” stent thrombosis was recorded according to the Academic Research Consortium of Circulatory System Devices Panel Meeting, an advisory committee to the US Food and Drug Administration (FDA) in 2006.
2.4 Statistical analysis
Continuous variables were expressed as mean ± SD (SD: standard deviation) or the median and interquartile range, and they were compared using the independent t test or Mann-Whitney U test between the two groups. Categorical variables were compared with Pearson’s Chi-square or Fisher’s exact tests between the two groups. Multivariate logistic regression analysis was performed to identify an independent predictors of clinical outcomes. Clinical variables were included this analysis for adjustment. All statistical tests were 2-tailed, and a p value < 0.05 was considered statistically significant. Statistical analysis was done using the SPSS version 18.0 (SPSS, Inc., Chicago, IL).
To adjust for the bias inherent to the decision of choosing PCI alone or PCI with TA group, propensity scores were used. Matching was performed using "many-to-one” individual matching between PCI alone and PCI with TA groups.
3.1 Baseline characteristics
A total of 3749 patients were enrolled in the current study. Enrolled patients were divided into 2 groups according to use of TA during PCI: PCI with TA group (n=1630) and PCI alone group (n=2119). TA during PCI were performed in 43.7 percent of total patients.
Patients in PCI with TA group were younger and higher BMI. In laboratory data, Creatinine clearance, HDL level were significantly higher in PCI with TA group. In hemodynamic and procedural characteristics, more patients of PCI with TA group were with lower Killip class, door to balloon time and heart rate admission. PCI with TA group had more right coronary artery disease as the infarct-related vessel. Many more cases of single vessel diseases existed and more culprit only PCI was done in PCI with TA group. Glycoprotein IIb/IIIa inhibitor was more used in 29.3 percent of patients of PCI with TA group than PCI alone group. After propensity-score matching, there is no significant differences in clinical variable. But level of HDL and CK-MB were higher in PCI with TA group. Many more cases of transfemoral vascular approach in PCI alone group. Also glycoprotein IIb/IIIa inhibitor was more used in PCI with TA group than PCI alone group after propensity-score matching.
3.2 Clinical outcomes in all patients
Unadjusted and adjusted one-year clinical outcome before and after propensity matching are shown in table 1.

Adjust included various clinical Variables including age, sex, BMI, heart rate at admission, SBP at admission, HDL, Creatine clearance, Hemoglobin, symptom balloon time (min), index procedure (culprit only PCI vs. Multi-vessel PCI), use of statin, beta-blocker, RAS blocker, Glycoprotein IIb/IIIa inhibitor, LVEF, .
MACE and all-cause mortality were occurred in 435(11.6%) and 271(7.2%) patients during one-year follow up. With respect to the primary efficacy outcome, there was no significant difference in the incidence of MACE between PCI alone and PCI with TA group (8.4% vs. 7.9%, unadjusted Odd ratio (OR) with 95% confidence interval (CI) 0.925 [0.737-1.160], p value=0.499 for TA use). Also, after propensity-score matching, there were no significant differences in the incidence of one-year MACE between the two group (8.2 % vs. 8.2%, adjusted OR with 95% CI 1.187 [0.863-1.633], p value=0.291 for TA use). The secondary efficacy outcome, CVD and all-cause mortality were not different between the two groups. Also, after propensity-score matching, there were no significant differences in the incidence of one-year CVD and all-cause mortality between the two groups. (CVD; 6.0 % vs. 5.8%, adjusted OR with 95% CI 1.222 [0.778-1.920], p value=0.523 for TA use, all-cause mortality; 7.3 % vs. 7.1%, adjusted OR with 95% CI 1.130 [0.776-1.647], p value=0.523 for TA use)
3.3 Clinical outcomes in subgroup
Subgroup analysis of composite of CVD, recurrent MI and stroke in propensity score matching patient.
Subgroup analysis suggests that the impact of PCI with TA did not clinically relevant in mortality of all patient with PCI at one-year. So, PCI wih TA was no efficacy of clinical outcome at one-year in subgroup analysis.
Our study was conducted to determine if PCI with TA expected to be effective in patients with total occlusion of coronary artery could reduce cardiac mortality in Korean patients with STEMI.The major finding of our study is that thrombus aspiration of patients with STEMI who were underwent primary PCI within 12 hours, pre-procedural TIMI flow 0,1 did not reduce the risk of the adverse clinical outcomes at one-year. Moreover, There was no efficacy of clinical outcome when subgroup analysis between the PCI with TA and PCI alone.
The result of our study was corresponded well with several large-scale trials. [7-9,14,15] In randomized clinical trial of Thrombus Aspiration in ST-Elevation Myocardial Infarction in Scandinavia (TASTE), routine thrombus aspiration before PCI did not reduce 30-day mortality, and rate of death from any cause or the composite of death from any cause, re-hospitalization for myocardial infarction, or stent thrombosis at 1 year [8,9]. The Trial of Routine Aspiration Thrombectomy with PCI versus PCI Alone in Patients with STEMI (TOTAL) also pointed out that the thrombus aspiration did not significantly improve cardiovascular mortality in 180 days. Rather, the TOTAL trial found that the risk of stroke in the patients treated thrombus aspiration was significantly higher within 30 days. [7]
However, the previous several reports disagreed with our findings. In TAPAS trial [3], 1-year cardiac death was reduced in TA group (HR:1.93; 95% CI [1.11-3.37], p=0.020). Burzotta et al. [6] showed in individual patients-data pooled analysis of randomized studies that thrombectomy significantly improved the clinical outcome in patients with STEMI undergoing mechanical reperfusion. Also Cistopoulos et al. [2] documented that the use of manual thrombectomy devices is associated with significant improvements in ST-segment resolution, Myocardial Blush Grade (MBG) 3, TIMI grade 3 flow as well as clinical parameters (43% reduction in mortality, p=0.04) in patients undergoing primary PCI.
A few KAMIR data demonstrated that TA showed clinical benefit only in special subgroups. Hachinohe et al. [16] compared clinical outcomes between PCI with TA and PCI alone group. Although TA was not enhanced clinical outcomes in all patients, TA for LAD occlusion and use of GP IIb/IIIa inhibitor with TA showed an improvement of 12-month MACE. Sim et al. [17] also reported that manual TA during primary PCI was not improved clinical outcomes at 12 month, and it may become clinically relevant with longer total ischemic time, forming a U-shaped relationship.
The use of glycoprotein IIb/IIIa inhibitor and manual thrombectomy had debates in some studies. [6,16,18,19] In Intracoronary Abciximab and Aspiration Thrombectomy in Patients With Large Anterior Myocardial Infarction (INFUSE-AMI) trial, an intracoronary bolus of the glycoprotein IIb/IIIa inhibitor abciximab was effective in reducing the infarct size, whereas thrombectomy by means of manual aspiration was not. Reduced embolization and improved myocardial perfusion may improve clinical outcomes. Similar result also report based on Korean patients that manual TA was not associated with reduced infarct size assessed by cardiac computed tomography [20]. TA may not be a safe procedure and distal embolization including cerebral embolization can occur [7,15]. Coronary thrombus material triggers thrombotic, inflammatory, vasoconstrictor, and other pathways, and evacuating a portion of the thrombus and plaque material addresses only a part of the pathophysiological problem. Disrupting thrombus formation pharmacologically may be more effective [8].
Recently, on the basis of the results of the INFUSE-AMI, TASTE and TOTAL trial, The ACC/AHA guidelines 2015 have been revised that the usefulness of selective and bail-out aspiration thrombectomy in patients undergoing primary PCI is not well established (Class IIB, level of evidence C). Also, routine aspiration thrombectomy before primary PCI is not useful (Class III, level of evidence A) [21]. Routine thrombus aspiration is not recommended (Class III, level of evidence A), but in cases of large residual thrombus burden after opening the vessel with a guide wire or a balloon, thrombus aspiration may be considered in ESC guideline 2017. [22]
Although our study is analyzed only based on one-year events, our results didn’t show any benefit of TA during PCI. Moreover, TA in patients with long ischemic time or TA with concomitant use of Glycoprotein IIb/IIIa inhibitor were not enhanced clinical outcomes. There results implied the probability that TA might be performed in patients with larger burden of thrombus or in patients with higher risks, and resulted in worse clinical outcomes.
Types of thrombus can affect mortality during PCI. Some studies have focused on the macroscopic appearance of the aspirated material, subdividing into white (fibrin-rich) and red (erythrocyte-rich) thrombus. White thrombus was typically found in patients with a small thrombus burden and a short ischemic time. By contrast, red thrombus tended to be aspirated from late-presenting patients who had a higher risk of distal embolization and cardiac mortality. [23] In our study, we could net analyze the type of thrombus.
This study has several limitations. First, although this study was conducted in the patients with MI registered with the KAMIR-NIH and statistical adjustment was performed, some confounding factors may still exist. Second, we used TIMI flow grade, but it is a subjective one based on gross examination and there was no information about other markers of myocardial perfusion such as corrected TIMI frame count, myocardial brush grade which are known to more precisely associate with prognosis. [24,25] Third, as we analyzed only about one-year events, our study might be underpowered to demonstrate the clinical usefulness of TA in STEMI patients.
Our study shows that routine thrombus aspiration during primary PCI as compared with PCI alone did not reduce MACE and all-cause mortality among patients with STEMI and pre-procedural TIMI flow 0,1 at one-year.
It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,

Dear Maria Emerson, Editorial Coordinator of International Journal of Clinical Case Reports and Reviews, What distinguishes International Journal of Clinical Case Report and Review is not only the scientific rigor of its publications, but the intellectual climate in which research is evaluated. The submission process is refreshingly free of unnecessary formal barriers and bureaucratic rituals that often complicate academic publishing without adding real value. The peer-review system is demanding yet constructive, guided by genuine scientific dialogue rather than hierarchical or authoritarian attitudes. Reviewers act as collaborators in improving the manuscript, not as gatekeepers imposing arbitrary standards. This journal offers a rare balance: high methodological standards combined with a respectful, transparent, and supportive editorial approach. In an era where publishing can feel more burdensome than research itself, this platform restores the original purpose of peer review — to refine ideas, not to obstruct them Prof. Perlat Kapisyzi, FCCP PULMONOLOGIST AND THORACIC IMAGING.
