
Research Article | DOI: https://doi.org/10.31579/2690-1919/119
1 Department of Ophthalmology, College of Medicine, University of Nigeria Teaching Hospital Ituku-Ozalla, Enugu, Nigeria.
*Corresponding Author: Stella Ngozi Onwubiko, Department of Ophthalmology, College of Medicine, University of Nigeria Teaching Hospital Ituku-Ozalla, Enugu.
Citation: Stella Ngozi Onwubiko, Nkiru Zuada Nwachukwu, Chioma Nwabugwu Ehumadu, Factors Associated with and Reasons for Loss to follow-up Among Glaucoma patients at a Nigerian eye Hospital. J Clinical Research and Reports, 5(5); DOI:10.31579/2690-1919/119
Copyright: © 2020 Stella Ngozi Onwubiko. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 August 2020 | Accepted: 16 September 2020 | Published: 21 November 2020
Keywords: loss to follow-up; glaucoma; Nigeria
Background: Glaucoma is an emerging vision-threatening disease requiring a life-long management protocol with regular surveillance.
Aim: To explore the factors associated with and reasons for loss to follow-up among glaucoma patients.
Methods: All adult glaucoma patients who attended Bridget medical Centre (BMC) Eye hospital, Enugu during a two-year period (2016 – 2018) were identified via the medical records. Those who had missed an appointment by at least 12 months were reached via their cellular phones to ascertain their reasons. Information on their socio-demographic and clinical characteristics was retrieved from their records. Data was analyzed using SPSS version 21. Chi-square test was done to identify the factors associated with loss to follow-up. The level of significance was at p< 0.05.
Results: A total of 113 patients had glaucoma. They were mainly males, 67(59.3%), retirees with a mean age of 62.0±2SD years. Ninety-four (83.2%) participants were lost to follow-up. The main reasons were forgetfulness, 33(41.2%), and have not noticed any problem in vision, 20(25.0%).
Male gender, advanced age, tertiary education, retiree, normal visual acuity, moderate/advanced stage, IOP of less than 21mmHg, more than 5 years of diagnosis and using more than one medication were associated with loss to follow-up. However, only Retiree and IOP of less than 21mmHg were statistically significant.
Conclusion: The findings from this study emphasized the need for continual glaucoma education and appointment reminder, especially to Retirees with normal intraocular pressure.
Globally, glaucoma is the commonest cause of avoidable, irreversible blindness, with an estimated prevalence of 3.54%. [1] Projections from 2013 into 2040 showed an increase by 74% from 64.3 million to 111.8 million of the global number of people with glaucoma, affecting Africans and Asians disproportionally [1].
Glaucoma is an emerging vision-threatening disease requiring a life-long management protocol with regular surveillance. Documented evidence has shown that while adherence to therapy and appointment schedule delay glaucoma disease progression and reduce vision loss,[2, 3] poor follow up is associated with glaucoma severity and the risk of blindness. [4] However, patients’ adherence with glaucoma follow-up remains a global challenge, with varying rates of loss to follow-up regimen ranging from 3.6% to 60.5% [3, 5, and 6].
Possible factors associated with glaucoma follow-up have been explored across the globe. Male gender,[3] younger age [5, 6], black race [7], mild glaucoma disease [6],lower intraocular pressure [3],lack of formal education [8] and no health insurance [5] were linked with loss to follow-up. Poor understanding of the importance of regular follow-up [3, 8, 9], appointment schedule difficulties [9], long waiting time [9], systemic co-morbidities [9], and lack of accompanying person [8] were the documented reasons for loss to follow-up.
An in-depth understanding of these determinants of non-adherence with glaucoma follow-up offers a useful guide for intervention measures that could improve patients’ clinical outcomes among the studied population. The fore-going background therefore underscores the need for this survey in the study area, which predominantly harbors the ethnic Ibos, a documented risk factor for glaucoma blindness [10].
Background: this study was carried out at the BMC Eye hospital, a private eye specialist hospital located in Enugu state Nigeria, within the tropical rainforest climatic zone. It is staffed by consultant ophthalmologists / subspecialists, optometrists, ophthalmic technicians, and ophthalmic nurses. It provides inpatient and outpatient promotive, preventive, curative and rehabilitative eye care services to the inhabitants of Enugu state and beyond.
Subjects: consecutive, consenting 113 glaucoma patients, aged 18 years and above, who met with the eligibility criteria within the study period, January 2016 to December, 2018.
Eligibility criteria: Glaucoma patients who had missed an appointment by at least 12 months and voluntarily gave informed consent to participation.
Ethics: Prior to the start of the study, ethics clearance compliant with 1964 Helsinki Declaration was obtained from Health Research Ethics Committee (HREC) of the University of Nigeria Teaching Hospital Ituku-Ozalla Enugu (Institutional Review Board).
Study design: This was be a cross-sectional, descriptive, hospital-based survey involving 113 glaucoma patients, who had missed an appointment by at least 12 months. Participants were reached via their cellular phones to ascertain their reasons. Information on their socio-demographic and clinical characteristics was retrieved from their records.
Study instruments: the pre-tested questionnaire comprised of three sections: socio-demography, clinical profile and reasons for loss to follow-up.
Study procedure: The medical records of glaucoma patients who attended the hospital from January 2016 to December, 2018 were retrieved. Participants who had missed an appointment by at least 12 months were identified and reached on phone to ascertain their reasons for loss to follow-up. Following a voluntary informed consent, the study questionnaire was administered after documenting the following parameters from the records: visual acuity (VA), perimetry, pachmetry, gonioscopy, tonometry, and optic disc assessment with +90D lens, as well as number of medications in use. The clinical examinations were done by the glaucoma specialist.
VA was done with the log MAR chart. Visual field assessment was done with static automated perimetry (SAP), (Humphrey Visual Field Analyzer 30-2; Humphrey Instruments, San Leandro, California, USA) using a 30-2 threshold program (HFA30-2) with the SITA Standard strategy. The Goldmann applanation tonometer (Haag-Streit 900; Haag Streit, Koeniz, Switzerland) was used to measure the intraocular pressure of each participant in the mornings between 8am and 10am. Gonioscopy was done using a four-mirror goniolens, while optic disc examination was done with +90D lens. The severity of glaucoma was staged according the guidelines of the American Academy of Ophthalmology.
Study definitions
Loss to follow-up: missing an appointment by at least 12 months
Mild or early stage glaucoma: optic nerve head abnormalities consistent with glaucoma, but no current defect on the visual field with SAP.
Moderate stage: optic nerve abnormalities consistent with glaucoma and glaucomatous visual field abnormalities in one hemifield and not within 5 degrees of fixation
Severe stage: optic nerve abnormalities consistent with glaucoma, glaucomatous visual field abnormalities in both hemifields and/or loss within 5 degrees of fixation in at least one hemifield.
Data management
Data was cleaned, edited, coded and analysed using the Statistical Package for Social Sciences (SPSS) software for windows, version 21.0 (SPSS Inc., Chicago, Illinois, USA). It was categorised into socio-demographic variables and clinical profile and subjected to descriptive statistical evaluation to yield frequencies, percentages, and proportions. Bivariate analysis was used to identify the factors associated with loss to follow up. The level of significance was placed at p- value of < 0.05.
A total of 113 patients had glaucoma. They were mainly males, 67(59.3%), married, retirees with tertiary education and a mean age of 62.0±2SD years. See table 1.

Table 1: Socio-demographic characteristics of participants. N = 113
The majority had moderate/advanced stage of primary open angle glaucoma, for more than 5 years, with a mean intraocular pressure (IOP) of 20 ±9 mmHg.
Ninety-four (83.2%) participants were lost to follow-up, among whom 80(85.1%) were successfully reached on phone.
Male gender, age 70 years and above, tertiary education, retiree, normal visual acuity, moderate/advanced stage, IOP of less than 21mmHg, more than 5 years of diagnosis and using more than one medication were associated with loss to follow-up. However, only retiree and IOP of less than 21mmHg were statistically significant. Table 2.
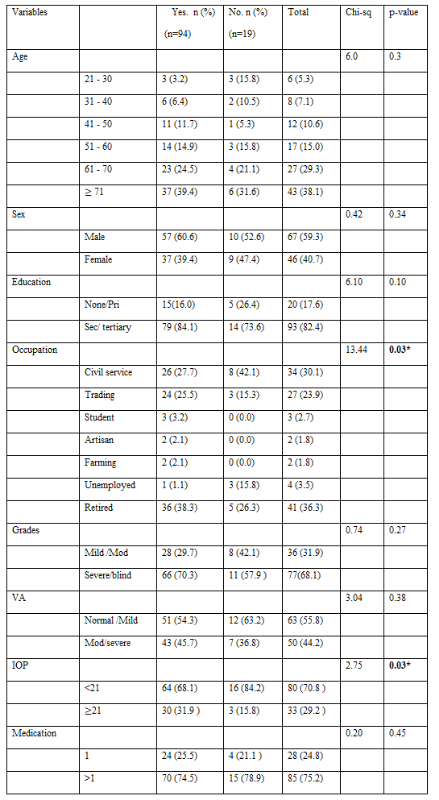
*significant, pri = primary, sec = secondary, mod = moderate.

Table 2: Factors associated with loss to follow up. N = 113
The main reasons for loss to follow-up were forgetfulness, 33(41.2%), and have not noticed any problem in vision, 20(25.0%). Table 3.
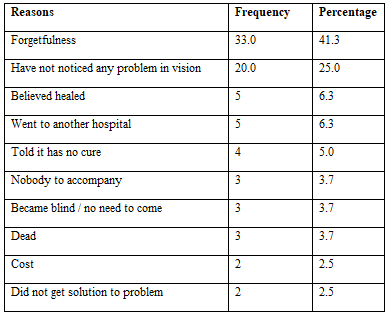

Table 3: Reasons for loss to follow-up. N = 80.
Glaucoma is an emerging vision-threatening disease requiring a life-long management protocol with regular surveillance. In this study, 83.2% of the participants were lost to follow-up. This is comparable with 86.5% reported in the rural south India [11], but contrasts with 3.6% in Seoul Korea [3] and other reports made elsewhere in Nigeria [6] and the USA [4]. The variations in the study definitions, participants’ socio-demographic and clinical characteristics may explain this disparity among studies. Nonetheless, interventions aimed at upholding adherence to glaucoma follow-up should get a global attention in order to reduce the burden of irreversible, though avoidable glaucoma blindness.
In this study, retiree and IOP of less than 21mmHg were significantly associated with loss to follow-up. This is consistent with the observation made in Seoul Korea [3] but contrasts with an American study [12], where the advanced age group were adherent to the appointment schedule. In contrast as well, Ngan et al [5] reported an association between the younger age group with loss to follow-up. The Retirees usually have chronic, systemic co-morbid conditions such as diabetes mellitus and, heart diseases to spend on. In this study background, where health insurance is not universally accessible, the cost of treatment therefore becomes so exorbitant and in the end, the eye medications are not bought and the follow up visits are abandoned entirely. Restructuring the health insurance scheme to accommodate all citizens irrespective of their job status is therefore advised. Government should as well make adequate provision in the health budget to cater for these vulnerable groups.
The main reasons for loss to follow-up were forgetfulness and have not noticed any problem in vision, in this study. The south Indian study [8] comparably made similar observations in addition to lack of escort. Contrarily, in the USA [9], long waiting time, difficulty in scheduling appointment, and systemic co-morbidities while in Seoul Korea [3], poor understanding and unawareness were the reported barriers and reasons for inconsistent follow-up. Given these reasons, the need for continual glaucoma patients’ counselling and appointment reminder via telephone calls or text messages to patients’ relatives cannot be underestimated in the study area.
The findings from this study emphasised the need for continual glaucoma education and appointment reminder, especially to Retirees with normal intraocular pressure.
Declarations / Compliance with Ethical Standards
None.
The authors declare that they have no conflict of interest.
This was obtained from the ethics committee of University of Nigeria Teaching Hospital Enugu. The procedures used in this study adhere to the tenets of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent: informed consent was obtained from all individual participants included in the study.
Data availability: Available.
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by the authors. The first draft of the manuscript was written by [Stella Ngozi Onwubiko] and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
