
Research Article | DOI: https://doi.org/10.31579/2690-1897/223
1Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre, 191014, Mayakovskogo st., 12, Saint-Petersburg, Russia.
2Department of Pathology with a course of forensic medicine named after D.D. Lochov, St. Petersburg State Pediatric Medical University, 194100, Litovskaya st., 2, Saint-Petersburg, Russia.
3The North-Western State Medical University named after I.I. Mechnikov, 191015, Kirochnaia st., 41, Saint-Petersburg, Russia.
*Corresponding Author: Darya Sitovskaya, Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre, 191014, Mayakovskogo st., 12, Saint-Petersburg, Russia.
Citation: Darya Sitovskaya, Artur Akopyan, Tatyana Sokolova, Yulia Zabrodskaya, (2024), Expression of the Tight Junction Protein Claudin in the Blood-Brain Barrier in the Temporal Lobe of Patients with Drug-Resistant Epilepsy, J, Surgical Case Reports and Images, 7(10); DOI:10.31579/2690-1897/223
Copyright: © 2024, Darya Sitovskaya. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 November 2024 | Accepted: 11 November 2024 | Published: 18 November 2024
Keywords: epilepsy; drug-resistant epilepsy; blood-brain barrier; tight junctions; claudin
Epilepsy is a major global health issue, and despite the availability of antiepileptic drugs, more than 30% of patients develop drug-resistant epilepsy and require surgical treatment. It is now known that disruption of the blood-brain barrier (BBB) is one of the manifestations of this disease, and in animal studies, the severity of epileptic seizures correlates with the degree of BBB disruption. Changes in the tight junctions of endothelial cells, specifically in the amount of claudin protein, which is a key component of the BBB, are of great interest.
The purpose of this study was to investigate claudin immunoreactivity in the cerebral cortex and white matter of patients with drug-resistant epilepsy (DRE).
Materials and Methods: Biopsy material from fragments of the temporal lobe was obtained intraoperatively from 15 patients (5 women, 10 men) with locally-caused DRE, aged 20 to 42 years with an average age of 28.7 years. Autopsy material from 6 patients who died from somatic diseases and had no history of neurological disorders was used as a comparison group. Histological sections stained with hematoxylin and eosin, as well as immunohistochemical (IHC) reactions with antibodies to claudin, were studied. The results of the IHC reactions were assessed by calculating the densitometric density of stained basement membranes of vessels in 10 fields of view of the cortex and white matter of the resected temporal lobe in each patient. Statistical analysis was carried out using the Statistica v.10 program, and a difference was considered significant at p<0.05.
Results: Histological analysis revealed focal cortical dysplasia in all patients. IHC reactions with claudin showed varying degrees of immunopositivity in the vascular endothelium of patients with DRE, with some cases showing complete loss of claudin. In the cortex, the level of claudin expression ranged from 0.072 to 0.554 (mean = 0.267 ± 0.088), and in the white matter, it ranged from 0.048 to 0.528 (mean = 0.181 ± 0.064). Statistical analysis showed no significant difference in claudin expression between patients with drug-resistant epilepsy and the comparison group (p-value = 0.43). However, a significant difference was found in the cortex according to the Mann-Whitney U test (p-value = 0.01). A correlation analysis using Spearman's correlation coefficient revealed a medium-strength negative correlation.
Conclusion: In patients with drug-resistant epilepsy, there is a decrease in claudin-5 immunoreactivity in the cerebral cortex. Defects in tight junction proteins, with a predominant effect on cortical vessels, may be both a primary and secondary factor in epilepsy and could potentially be a therapeutic target in this group of patient.
Epilepsy is a major global health issue, with more than 30% of patients developing drug-resistant forms of the disease that require surgical treatment [1]. Like many other neurological disorders, epilepsy is associated with dysfunction of the blood-brain barrier (BBB) [2]. The BBB serves as a protective layer in the central nervous system, regulating the exchange of molecules between the blood and the brain microenvironment [2]. It is composed of several components, including vascular endothelial cells and tight junctions [3]. Enzymes also play a role in altering the structure of drugs and neurotransmitters, making it difficult for them to cross the BBB [3]. While endothelial cells are the main component of the BBB, pericytes, astrocytes, and the basement membrane also contribute to its barrier functions [4]. The tight junctions between endothelial cells are particularly important in maintaining the integrity of the BBB. These junctions are made up of various proteins, including claudins, occludin, junctional adhesion molecules (JAMs), and endothelial selective cell adhesion molecules (ESAMs), as well as intracellular proteins such as zonula occludens (ZO-1/2) [5]. Other proteins, such as cingulin, 7H6, Afadin, and JACOP, connect ZO-1 to the cytoskeleton [5]. There are different types of claudin proteins, with claudin-5 being the most abundant in the BBB [6]. It has been shown that one endothelial cell can express up to 18 million claudin-5 molecules [6]. Damage to the BBB can both contribute to and result from various pathological processes in the brain, including epilepsy.
Purpose of the study. To investigate the expression of claudin-5 in the cerebral cortex and white matter of patients with drug-resistant epilepsy.
Biopsy samples from fragments of the temporal lobe of the brain were retrospectively studied at Polenov Neurosurgical Institute – Branch of Almazov National Medical Research Centre. The samples were obtained intraoperatively from 15 patients (5 women, 10 men) with locally caused EEG, aged 20 to 42 years with an average age of 28.7 years. The area of the epileptic focus was determined using MRI, PET-CT, and EEG with invasive monitoring. Autopsy samples from 6 patients who died from somatic diseases and had no history of neurological disorders were used as a comparison group. Of these, 1 was a woman and 5 were men, with an average age of 51 years. The samples were fixed in 10% buffered formalin, dehydrated, and embedded in paraffin. Histological sections were stained with hematoxylin and eosin, and immunohistochemical (IHC) reactions were performed using antibodies to claudin-5 and CD31 (antibodies from Diagnostic Biosystems, USA, EnVision imaging system). Antibodies to CD31 were used to confirm the localization of markers in the vascular endothelium. Histological analysis and microphotography were performed using a Leica DM2500 M microscope equipped with a DFC320 digital camera and IM50 image manager (Leica Microsystems, Wetzlar, Germany). The results of the reactions were assessed by calculating the densitometric density of stained basement membranes of vessels in 10 fields of view of the cortex and white matter of the resected temporal lobe in each case (PhotoM, Russia). The program calculates the densitometric density relative to background areas (symb. units, s.u.). Data are presented in the format M ± m (arithmetic mean ± standard error). Statistical analysis was carried out using the Statistica v.10 program. Since a normal distribution was not obtained, nonparametric statistical methods were used for analysis, and a difference was considered significant at p<0>
Upon studying the histological material, focal cortical dysplasia (FCD) was verified in all patients, with the most common variant being FCD type Ic with impaired tangential and radial lamination (7 cases, 46.7%). IHC reactions with claudin showed immunopositivity in the walls of blood vessels of varying severity: from weak to moderate in patients with DRE (Figure. 1, A-B). A decrease in the density of endothelial staining was observed in both the cortex and white matter, with some foci showing complete loss of staining. In comparison, the expression was strong and uniform in the comparison group (Figure. 1, C-D).
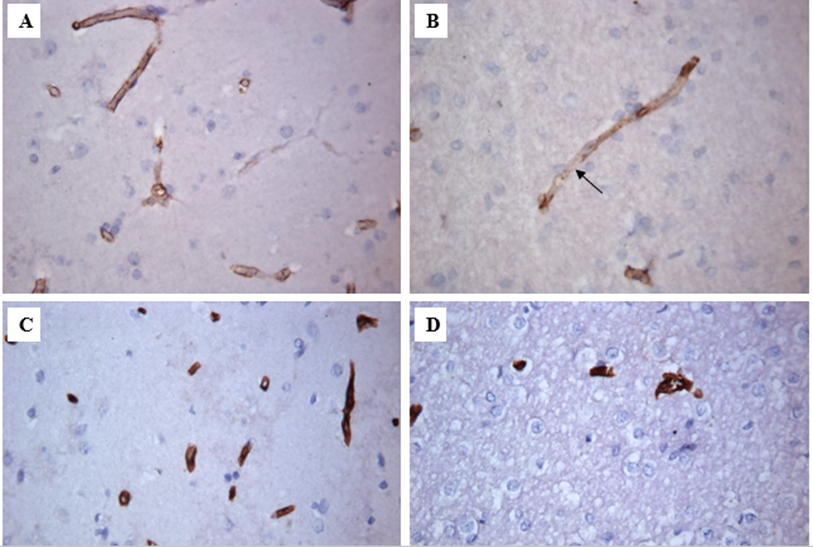
Figure 1: Claudin expression in the cortex and white matter of the temporal lobe of patients with DRE and in the comparison group (description in the text).
Immunohistochemical reaction, ×400
A – Cortex of a patient with epilepsy.
B – White matter of a patient with epilepsy. Areas of loss of staining are indicated by an arrow.
C – Cortex of the patient in the comparison group.
D – White matter of the patient in the comparison group.
A study was conducted to examine the densitometric density of claudin-positive vessels in the cortex and white matter of the temporal lobe in patients with DRE. The results showed that in the cortex, the level was from 0.072 to 0.554 (μ = 0.267 ± 0.088), and in the white matter, it was from 0.048 to 0.528 (μ = 0.181 ± 0.064). In comparison, the densitometric density of claudin in similar areas studied in patients in the control group was from 0.112 to 0.465 (μ = 0.302 ± 0.07) in the cortex and from 0.142 to 0.391 (μ = 0.264 ± 0.06) in the white matter. Statistical analysis revealed that there was no significant difference in claudin expression in the white matter between patients with DRE and the control group (p-value = 0.43). However, there was a significant difference in the cortex according to the Mann-Whitney U test (p-value = 0.01) (Fig. 2, A-B).
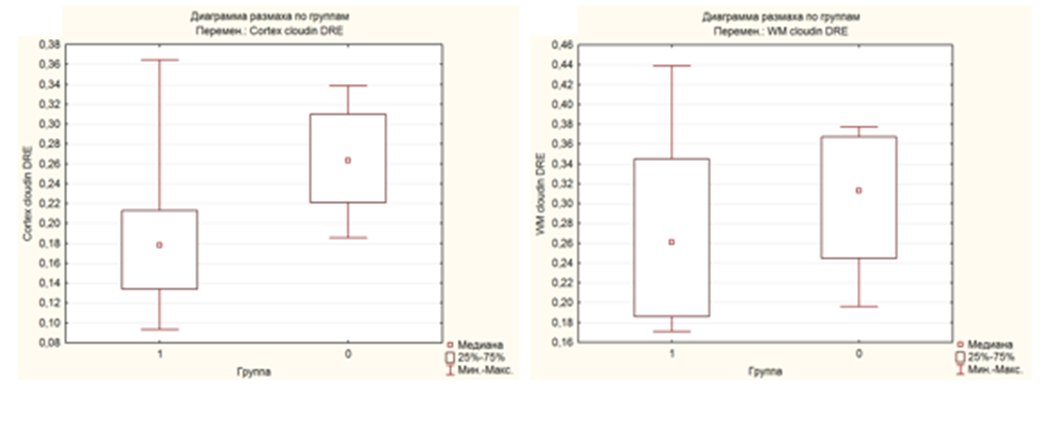
Figure 2: Range diagram of data claudin expression in the cortex (A) and white matter (B) of the temporal (explanation in the text). Group 1 – patients with DRE, 0 – patients in the comparison group.
A correlation analysis was also conducted between the levels of claudin expression in the cortex and white matter of patients with DRE, which showed a Spearman correlation coefficient of -0.56. According to the Chaddock scale, this indicates a negative moderate strength relationship (Fig. 3).
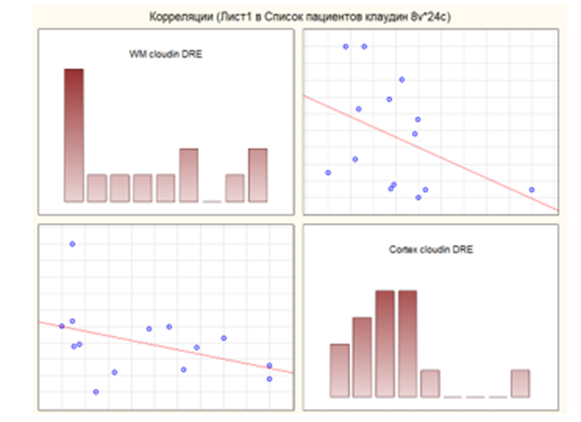
Figure 3: Correlation analysis between the level of claudin expression in the cortex and white matter of the temporal lobe of patients with DRE.
BBB dysfunction is a hallmark pathology of many neurological diseases. However, establishing a cause-and-effect relationship between the destruction of the BBB and the development of pathology is challenging. While there is a significant amount of data supporting the link between seizures and disruption of the BBB, the exact relationship between the two remains unclear. For instance, a study on rats with epilepsy showed that increasing the permeability of the BBB with mannitol led to an increase in the frequency of seizures [7]. However, this effect was only observed in some rats, while others showed no change or a return to the original level of seizures. Additionally, there is evidence that damage to the BBB may be a contributing factor in the development of seizures. In one study, a quarter of patients experienced seizures immediately after the BBB was disrupted [8]. There are several potential mechanisms by which BBB disruption may lead to epilepsy [9]. For example, increased permeability can allow blood albumin to enter brain tissue, where it can be taken up by neurons, astrocytes, and microglia. This can lead to downregulation of potassium channels in astrocytes, activation of NMDA receptors, and hyperexcitability. Albumin uptake by neurons can also result in cell death. Furthermore, the presence of albumin in the brain can induce transcriptional changes in genes such as transforming growth factor (TGF-β), which can increase inflammation and contribute to hyperexcitability [9]. The claudin-5 protein is a member of the claudin family, which consists of 27 characterized members in mammals [10]. It is encoded by the CLDN5 gene, located on chromosome 22 in humans. Mutations in this gene have been linked to developmental delay, seizures (primarily infantile-onset focal epilepsy), microcephaly, pontine atrophy, and brain calcifications [11-12]. Claudin-5 is expressed in various tissues, with the highest levels found in the brain and lungs [13]. The protein has a molecular weight of 23 kDa and consists of four transmembrane domains, two extracellular loops (ECL1 and ECL2), one intracellular loop, and intracellular -NH2 and -COOH ends [2]. The first extracellular loop (ECL1) plays a crucial role in creating the barrier properties of tight junctions [14], while the second loop is involved in the interaction between claudins [15]. Claudins are divided into two groups based on the length of their C-terminus: "classical" and "non-classical" [16]. The "classical" group includes claudins 1-9, 14, 17, and 19, which have similar structures and short C-termini. The "non-classical" group includes claudins 10-12, 15, 16, 18, 21, and 24, which have long C-domains [17]. In some claudins (1, 2, 4, 5, and 16), the C-domain can be phosphorylated, which regulates barrier functions. For example, phosphorylation of claudin-5 in the BBB leads to decreased permeability, while in the lung epithelium, it increases permeability [18-19]. Additionally, claudin proteins have a PDZ-binding domain at the C-terminus, which allows them to bind to intracellular proteins such as ZO-1/2/3. The intracellular loop and C-domain also contain cysteine molecules, which are sites of palmitoylation, the significance of which is not fully understood [20]. The question remains: what happens to the claudin-5 protein during BBB dysfunction? Our study revealed an uneven distribution of claudin-5, with some areas showing partial or complete loss. In another study, brain tissue from individuals with DRE showed no significant difference in claudin-5 expression between damaged and adjacent areas. However, vessels in damaged areas showed either overexpression or underexpression, as well as distorted distribution of claudin-5 [21]. This suggests that the uneven distribution of claudin-5 may contribute to increased permeability and subsequent damage to brain structures. It is worth noting that mice lacking claudin-5 died within 10 hours of birth [22]. Another study on mice found that both epileptic seizures and a pre-existing decrease in claudin expression in blood vessels can lead to an increase in the frequency of seizures [6]. This suggests that a pre-damaged BBB may be a contributing factor in the development of seizures, and that subsequent seizures can further increase barrier permeability. These studies demonstrate that BBB damage, specifically decreased levels of claudin-5, is associated with the development of epilepsy. This suggests that increasing claudin-5 levels may be a potential treatment for epilepsy. In a study aimed at investigating the therapeutic properties of increasing claudin-5 expression, mice were injected with a drug that indirectly increases the formation of the protein [6]. The injections reduced the severity of seizures and helped stabilize the blood-brain barrier. However, there are still some challenges to consider. Should claudin expression be increased throughout the entire brain, or only in specific structures [23-25]? Additionally, our study found a statistically significant decrease in claudin-5 in the cortex, raising the question of whether increasing its expression in the white matter would also be beneficial. Furthermore, in some vessels of patients with DRE, an increase in protein expression was noted, but its distribution was uneven [21], highlighting the importance of not only the quantity, but also the correct distribution of claudin-5.
In conclusion, our study found a decrease in claudin-5 immunoreactivity in the cerebral cortex of patients with DRE. Defects in tight junction proteins, with a predominant impact on cortical vessels, may be both a primary and secondary factor in epilepsy and could potentially be targeted for therapeutic intervention in this patient population.
It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,

Dear Maria Emerson, Editorial Coordinator of International Journal of Clinical Case Reports and Reviews, What distinguishes International Journal of Clinical Case Report and Review is not only the scientific rigor of its publications, but the intellectual climate in which research is evaluated. The submission process is refreshingly free of unnecessary formal barriers and bureaucratic rituals that often complicate academic publishing without adding real value. The peer-review system is demanding yet constructive, guided by genuine scientific dialogue rather than hierarchical or authoritarian attitudes. Reviewers act as collaborators in improving the manuscript, not as gatekeepers imposing arbitrary standards. This journal offers a rare balance: high methodological standards combined with a respectful, transparent, and supportive editorial approach. In an era where publishing can feel more burdensome than research itself, this platform restores the original purpose of peer review — to refine ideas, not to obstruct them Prof. Perlat Kapisyzi, FCCP PULMONOLOGIST AND THORACIC IMAGING.
