
Case Report | DOI: https://doi.org/10.31579/2690-8794/098
Associate Professor, Medicine, Ad-din Women’s Medical College Hospital, Dhaka, Bangladesh.
*Corresponding Author: Richmond Ronald Gomes, Associate Professor, Medicine, Ad-din Women’s Medical College Hospital, Dhaka Bangladesh.
Citation: Richmond R Gomes (2021) Expanded Dengue Syndrome Presenting as Acute Pancreatitis J, Clinical Medical Reviews and Reports. 3(9); DOI: 10.31579/2690-8794/098
Copyright: © 2021, Richmond R Gomes, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 August 2021 | Accepted: 25 September 2021 | Published: 12 November 2021
Keywords: expanded dengue, dengue hemorrhagic fever, shock, pancreatitis, lipase
Dengue is a painful, debilitating mosquito-borne disease(female mosquitoes of the Aedes genus, principally Aedes aegypti)caused by any one of four closely related dengue viruses.It is endemic in tropical and subtropical continent. World health organization (WHO) currently estimates there may be 50 -100 million dengue infections worldwide every year with over 2.5 billion people at risk of dengue. Symptomatic dengue virus infection may manifests as undifferentiated fever, classical dengue fever (with or without unusual hemorrhages), and dengue hemorrhagic fever(with or without shock). Expanded dengue syndrome (EDS) was coined by WHO in the year 2012 to describe cases, which do not fall into either dengue shock syndrome or dengue hemorrhagic fever. The atypical manifestations noted in expanded dengue are multisystemic and multifaceted with organ involvement, such as liver, brain, heart, kidney, central/peripheral nervous system, gastrointestinal tract, lympho reticular system. Here we present a case of 35 years old female without any comorbidities who was serologically diagnosed with dengue developed severe upper abdominal pain on 2ndafebrile day and eventually diagnosed as acute pancreatitis both by raised serum lipase and ultrasonographic evidence of swollen pancreas. She was treated conservatively and improved. Thus, all clinicians should keep in mind the possibility of acute pancreatitis as a part of expanded dengue syndrome.
Dengue is an arboviral infection common in tropical countries, including South and Southeast Asia and Western Pacific regions [1]. It is caused by the dengue pathogen, which is an enveloped ribonucleic (RNA) virus, from the Flaviviridae family [2]. The infection caused by the dengue virus causes a wide spectrum of diseases that can be life-threatening, such as dengue with hemorrhagic manifestations and severe dengue triggering dengue shock syndrome. Severe dengue (dengue hemorrhagic fever-DHF and dengue shock syndrome-DSS) is a potentially deadly complication due to plasma leaking, fluid accumulation, respiratory distress, severe bleeding, or organ impairment. The World Health Organization (WHO) has coined the term-expanded dengue to describe cases, which do not fall into either dengue shock syndrome or dengue hemorrhagic fever. This has incorporated several atypical findings of dengue. In clinical practice, the occurrence of atypical presentation should prompt us to investigate for dengue. Various atypical complications of severe dengue are myocarditis, encephalitis, acute motor weakness, Guillane-Barre likesyndrome, acute liver failure, lupus erythematosus, hemophagocytic syndrome, acute kidney injury, acute pancreatitis, immune thrombocytopenic purpura, acalculus cholecystitis and so on [3]. It is critical that physicians who monitor dengue illnesses, should be aware and alert to these atypical manifestations [4]. We have come across varied presentations of dengue fever in clinical practice and the present article throws light on one of the atypical manifestations of dengue. Even in the modern era of medicine, presentation of an acute abdomen remains a challenge for the surgeon. Though acute pancreatitis (AP) is a common cause of acute abdomen, AP of infective etiology is relatively uncommon [5]. Here we report a 35 years old female withexpanded dengue syndrome presenting as with acute pancreatitis.
A 35 years old lady, school teacher, not known to have any diabetes mellitus, hypertension, coronary artery disease or bronchial asthma presented to us with the history of high grade, intermittent fever, severe headache, bodyache and retro orbital pain for 4 days, vomiting for several times and severe prostration for 1 day. She denied any altered consciousness, convulsion, cough, chest pain, palpitation, shortness of breath, abdominal pain or distension, burning micturition, joint pain. She had no recent history of travel of late. She lives in 1stfloor of her apartment and have hobby of gardening. His husband just recovered from dengue 1 week prior her illness. On examination, she was toxic, conscious, oriented febrile (temperature 102oF), with pulse 110 beats/min, with normal rhythm and volume, Blood pressure was 110/70 mm of Hg. There was diffuse blanching erythema, more prominent over trunk (Figure 1).There was no signs of meningeal irritation. Fundoscopy was normal. She was started treatment conservatively with intravenous fluids, anti-emetics and anti-pyretic. On the following day, she became afebrile with reduced intensity of vomiting, headache and bodyache with feeling of general wellbeing. As repeat complete blood count showed progressive leucopenia and thrombocytopenia she was monitored closely for evidence of dengue hemorrhagic fever. On 2nd afebrile day, she complained of diffuse non radiating upper abdominal pain and vomiting. Her bowel was moved. She also complained of pre-date menstruation. Repeat abdominal examination showed epigastric tenderness and ascites as evidenced by presence of shifting dullness without hepatomegaly. There was also evidence of bilateral pleural effusion. There was no active bleeding from any site but narrowing of pulse pressure(100/90 mm of Hg) with rapid thread low volume pulse(120 /min) was observed. So clinical diagnosis of dengue hemorrhagic fever was established. Serial complete blood count was done. Ultrasonography, serum amylase and lipase were advised.
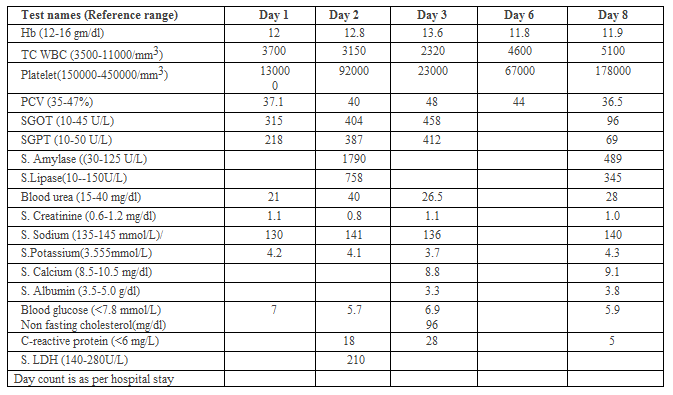
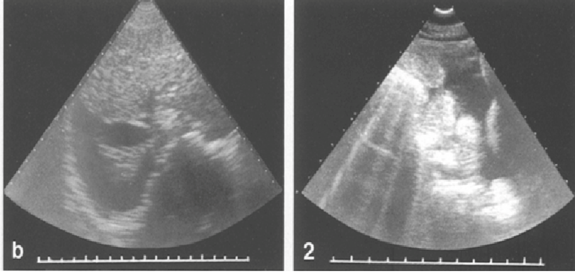
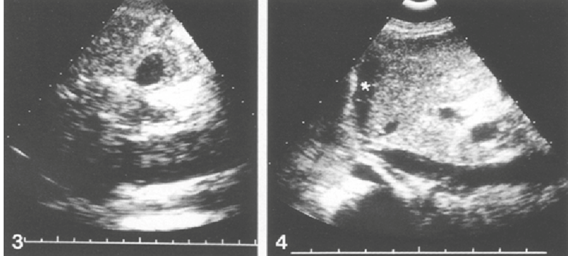
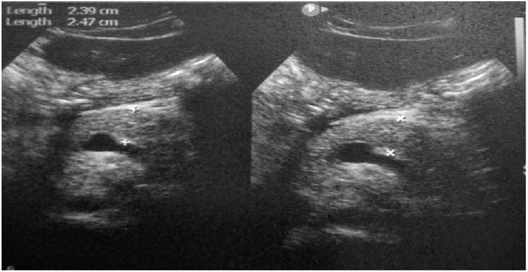
Ultrasonography of whole abdomen revealed ascites, bilateral pleural effusion (figure 2), thickened gall bladder wall and abnormal hepatic parenchyma (figure 3) and swollen pancreas (figure4).

Then she was labelled as acute pancreatitis as a spectrum of EDS. She was kept nothing per oral. Adequate isotonic crystalloid parenteral fluid, nasogastric feeding and opiate analgesic were started. She was transfused with one unit fresh whole blood. With conservative treatment she made a significant clinical recovery. On 8th day of her admission her clinical, hematological and biochemical parameters improved significantly. She was discharged from hospital on 10th day. On follow up at outpatient door after one week, she was asymptomatic apart from some post viral asthenia. Her amylase, lipase, SGPT, SGOT came within normal limit.
Dengue fever or break bone fever or Dacca fever which is a mosquito-borne tropical disease caused by the dengue virus which is an RNA virus of the family Flaviviridae; genus Flavivirus[6]. Symptoms typically begin three to fourteen days after infection [7]. These may include a high fever, headache, vomiting, muscle and joint pains, and a characteristic skin rash. Recovery generally takes two to seven days [6]. In a small proportion of cases, the disease develops into a more severe dengue hemorrhagic fever, resulting in bleeding, low levels of blood platelets and blood plasma leakage, or into dengue shock syndrome, where dangerously low blood pressure occurs [7].
Dengue is spread by several species of female mosquitoes of the Aedes genus, principally Aedes aegypti [7]. The virus has four serotypes [8, 9]; DEN 1, 2, 3, and 4.Iinfection with one type usually gives lifelong immunity to that type, but only short-term immunity to the others. Subsequent infection with a different type increases the risk of severe complications. A number of tests are available to confirm the diagnosis including detecting antibodies or antigens or direct viral culture.
Typically, people infected with dengue virus are asymptomatic (80%) or have only mild symptoms such as an uncomplicated fever [10-12]. Others have more severe illness (5%), and in a small proportion it is life-threatening. The incubation period (time between exposure and onset of symptoms) ranges from 3 to 14 days, but most often it is 4 to 7 days [13].
The characteristic symptoms of dengue are sudden-onset fever, headache (typically located behind the eyes), muscle and joint pains, and a rash. An alternative name for dengue, "breakbone fever", comes from the associated muscle and joint pains [14]. The course of infection is divided into three phases: febrile, critical, and recovery [15].
The febrile phase involves high fever, potentially over 40 °C (104 °F), and is associated with generalized pain and a headache; this usually lasts two to seven days [14, 15]. Nausea and vomiting may also occur. A rash occurs in 50–80% of those with symptoms in the first or second day of symptoms as flushed skin, or later in the course of illness (days 4–7), as a measles-like rash [16, 17]. A rash described as "islands of white in a sea of red" has also been observed [18]. Some petechiae (small red spots that do not disappear when the skin is pressed, which are caused by broken capillaries) can appear at this point, as may some mild bleeding from the mucous membranes of the mouth and nose. The fever itself is classically biphasic or saddleback in nature, breaking and then returning for one or two days [17, 18].
In some people, the disease proceeds to a critical phase as fever resolves [19]. During this period, there is leakage of plasma from the blood vessels, typically lasting one to two days. This may result in fluid accumulation in the chest and abdominal cavity as well as depletion of fluid from the circulation and decreased blood supply to vital organs. There may also be organ dysfunction and severe bleeding, typically from the gastrointestinal tract [19, 20]. Shock (dengue shock syndrome) and hemorrhage (dengue hemorrhagic fever) occur in less than 5% of all cases of dengue; however, those who have previously been infected with other serotypes of dengue virus ("secondary infection") are at an increased risk [20, 21]. This critical phase, while rare, occurs relatively more commonly in children and young adults [19].
The recovery phase occurs next, with resorption of the leaked fluid into the bloodstream. This usually lasts two to three days. The improvement is often striking, and can be accompanied with severe itching and a slow heart rate [15, 19]. Another rash may occur with either a maculopapular or a vasculitic appearance, which is followed by peeling of the skin. During this stage, a fluid overload state may occur; if it affects the brain, it may cause a reduced level of consciousness or seizures [20]. A feeling of fatigue may last for weeks in adults [25].
EDS is a terminology introduced by the WHO in 2012 to encompass the unusual manifestations of dengue involving severe damage to the liver, heart, kidneys or brain which do not fall into either dengue shock syndrome or dengue hemorrhagic fever. They may be related to underlying co-morbidities, associated co-infections or prolonged shock. Certain high-risk groups such as pregnant, infants, geriatric group, and patients with coronary artery disease, hemoglobinopathies and immunocompromised individuals are particularly susceptible to developing EDS. As clinicians, we must be aware of these atypical features so that we can suspect dengue early, especially during ongoing epidemics.
Acute Pancreatitis (AP) is an acute inflammatory process of the pancreas with varying involvement of other regional tissues or remote organs. While common causes of AP are gall stones and alcohol, infective agents also cause a small proportion of cases [22]. Viral infections that can cause pancreatitis are hepatitis B, hepatitis A, varicella, dengue, mumps .Pancreatitis in any infectious disease could be (a) definite pancreatitis if there is surgical or radiological evidence of pancreatitis, (b) probable pancreatitis if there is biochemical evidence in the form of more than three-fold elevated serum amylase or lipase and characteristic symptoms, or (c) possible pancreatitis if there is only asymptomatic biochemical evidence [23].
An infectious agent should be suspected as the cause of AP if the characteristic syndrome due to the infectious agent is present, which is seen in 70% of cases [24]. Criteria suggested for associating pancreatitis with an infective etiology include (a) finding the organism in pancreas or pancreatic duct, which is ‘definitive criteria’; (b) culture of the organism from the pancreatic juice or blood or serological evidence combined with characteristic clinical or epidemiological setting, which is ‘probable criteria’; and (c) culture of the organism from other body sites or serological evidence of infection, which is ‘possible criteria’ [25].
Abdominal pain is a common symptom (40%) in dengue infections and is more commonly associated with DHF. Some of the causes for abdominal pain in dengue infections include hepatitis, acute acalculous cholecystitis, acute pancreatitis, and colitis. Studies have reported the incidence of AP in dengue infections to be 14- 29% [26].
Till date, there have been only a few case reports of acute pancreatitis complicating DF from across the world. Our patient also had severe dengue which was complicated by acute pancreatitis which was evident by raised serum amylase and lipase and ultrasound findings. Hyperlipasemia and enlarged pancreas have been known to occur in DF; but acute pancreatitis is an atypical and rare presentation [27-29]. The exact pathogenesis of pancreatic involvement in dengue is not known. The physiopathology behind the acute pancreatitis in this infection is not well understood although there are two hypotheses that had better explain this process: (1) the pancreatic compromise of the biliary pathway and (2) the small hemorrhages in the peritoneal cavity. The first hypothesis suggests that the viral infection causes an autoimmune response to pancreatic islet cells, thus edema develops in the Vater's ampulla and obstructs the exit of pancreatic fluids [30]. The second hypothesis suggests that acute pancreatitis is caused by the direct inflammation and destruction of the pancreatic acinar by the same virus; this is mainly evidenced in dengue shock syndrome (grades III and IV of dengue hemorrhagic fever (DHF)) [31]. But it can be due to result of direct invasion by the virus itself causing inflammation and destruction of pancreatic acinar cells.
During a deep browse in the literature, we identified 15 articles reporting 17 patients with pancreatitis due to dengue fever. In summary, 76.5% (n=13) of cases were reported from Asia, 11.76% (n=2) from Latin America, and 5.9% (n=1) from Europe. Taiwan and Bangladesh were the countries with the highest reported cases, with 29.4% and 11.8%, respectively. The most prevalent serotype was DEN-1 in 64.71% of the cases and 35.3% of the cases did not report the serotype. The most frequent symptoms were fever (52.9%, nine cases), abdominal pain (47.1%, eight cases), vomiting (47.1%, eight cases), body pain (35.3%, six cases), chills (23.5%, four cases), and dyspnea (17.7%, three cases), and most of them were males (47.1%, eight cases). Regarding laboratory tests, 11.8% of the cases reported hypocalcemia, 41.2% had hyperlipasemia, 41.2% had hyperamylasemia, 35.3% had thrombocytopenia, 35.3% had dengue IgM and IgG positive detection, 11.8% had an NS1 positive antigen, 5.9% had edema of the thick gallbladder wall, 64.7% had low hematocrit, 5.9% had high pleural fluid amylase, 35.3% were dengue virus IgM positive and negative IgG, 5.8% of tests were of renal-derived function, 5.9% had lymphopenia, and 5.9% had hemoconcentration. About the pancreas examinations, 94.1% of the cases were diagnosed with pancreatitis with a CT scan and 5.9% reported hemorrhagic pancreatitis. The final diagnoses of the reported cases corresponded 64.71% to DHF grade I, 17.7% to DHF grade II, and 5.9% to DHF grade IV. In 70.6% of the cases, the patient was discharged, and 11.8% of them died.
Our patient never took alcohol or any offending drugs which could cause AP and had no gallstones on USG. The elevated enzymes, USG findings along with positive dengue NS1 antigen pointed towards the diagnosis on 2nd afebrile day. She was managed conservatively and improved dramatically. So far acute pancreatitis occurring during the critical phase of dengue has been reported.
Acute pancreatitis may be under diagnosed as a manifestation of dengue due to lack of awareness and it is likely that mild forms without any local and systemic complications may be missed. Therefore, clinicians might not request serum amylase or lipase or suspect the diagnosis despite patient having abdominal pain or vomiting. In patients with dengue fever who develops abdominal pain, it is helpful to estimate and monitor serum lipase and amylase levels and to perform abdominal imaging to rule out acute pancreatitis. Similarly, if the etiology of pancreatitis is not found and in the setting of fever and thrombocytopenia, it may be worthwhile working up for dengue fever even when fever has subsided. In all reported cases, the hyperlipasemia, hyperamylasemia, and dengue serological positivity were the tests that best detected dengue complicated with acute pancreatitis. The case is presented not only because of the rare presentation of a common disease but also to emphasize that in dengue endemic areas, the possibility of dengue related pancreatitis should be entertained in patients presenting with abdominal pain and fever. This will enable the patient to receive adequate monitoring and supportive care directed at the management of dengue along with the management of acute pancreatitis
None declared.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
