
Research Article | DOI: https://doi.org/10.31579/2834-5142/013
1 Lecturer – Nephrology - Faculty of Medical Sciences - UNIFACISA – PhD Student - Federal University of Pernambuco – Recife, Pernambuco, Brazil.
2 MD, PhD - Scientific Director – UNIFACISA - Campina Grande - Paraíba - Brazil.
3 Medical Student – UNIFACISA - Campina Grande - Paraíba - Brazil.
4 Nutricionist – Paraíba Endoscopic and Obesity Surgery Institution – ICOEP - Campina Grande - Paraíba - Brazil.
*Corresponding Author: Juliana Amaro Borborema Bezerra, Lecturer – Nephrology - Faculty of Medical Sciences - UNIFACISA. – PhD Student - Federal University of Pernambuco – Recife, Pernambuco, Brazil.
Citation: Borborema Bezerra JA, Carlos T. Brandt., Bezerra Borborema DM, Guilherme de Brito Lira Dal Monte and Florêncio Maciel FAM (2021). Does Bariatric Surgery Improve Kidney Function in obese Patients? A Cohort Study. International Journal of Clinical Nephrology. 3(1); DOI:10.31579/2834-5142/013
Copyright: © 2021 Juliana Amaro Borborema Bezerra. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 October 2021 | Accepted: 16 November 2021 | Published: 22 November 2021
Keywords: obesity; bariatric surgery; renal function; glomerular filtration rate; cystatin
Introduction: Obesity is a global epidemic that may cause renal dysfunction. Weight loss in the postoperative follow-up of bariatric surgery may improve renal function in these patients. Thus, the purpose of this study was to give insight on the subject using a sensible biomarker: cystatin C.
Materials and methods: This cohort was performed in the Obesity Department from Campina Grande – Paraiba, Brazil. It was recruited 35 obese (25 women and 10 men) who underwent bariatric surgery with follow-up of at least one year. The ages ranged from 24 and 57 years. Those with thyroid disease and with microalbuminuria ≥ 30mg/g were excluded. Serum levels of creatinine and cystatin C were measured, and the glomerular filtration rate (GFR) was estimated using the CKD Epi (Chronic Kidney Disease Epidemiology Collaboration) equation creatinine- cystatin C. The investigation was approved by the Ethics Committee. The sample was of convenience. Quantitative variables were expressed by the mean and standard deviation. Paired tests were used for assessing difference between means. Chi square test and exact Fisher were used for difference among frequencies. p ≤ 0.05 was used for rejecting the null hypothesis.
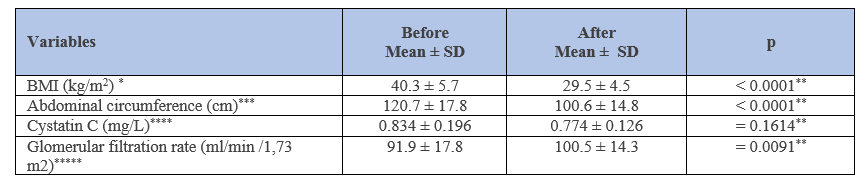
Results:The most frequent associated morbidities were: sexual dysfunction (n = 17 – 48.5%); hypertension (n =15 – 42.8%); type II diabetes (n =13 – 37.1%); anxiety (n = 14 – 40.0%); and depression (n = 12 – 34.2%). Twenty-three (65.7%) patients underwent sleeve technique and 12 (34.2%) bypass surgery. It was observed a significant reduction in the mean of body mass index (BMI) in the post-operative follow-up – p < 0.0001. The mean concentrations of cystatin C were similar, regarding to pre- and post-operative periods – p = 0.1614. There was a significant improvement of glomerular filtration rates - p= 0.0091. The improvement of renal function was more significant among those who underwent sleeve surgery as compared to bypass - p = 0.0008.
Conclusion: It was observed improvement of the majority of morbidities after bariatric surgery, as well as renal function, in obese individuals. Despite these results, larger and longer-term outcome cohorts are required for better answer of the main purpose of this health issue.
Obesity is an abnormal or excessive fat accumulation that may impair
health. It is most commonly assessed using body mass index (BMI), a simple and quick anthropometric tool that has a low cost. BMI ≥30 kg/m2 is considered obesity [1].
Obesity is a global epidemic, affecting all age, race and ethnic groups. Nowadays, overweight and obesity represent over one third of the planet population [2]. It increases the risk for many chronic diseases, such as diabetes mellitus, cardiovascular diseases, cancers and chronic kidney disease (CKD), which may impair renal function [3-9].
Inflammations, oxidative stress and hyper activation of renin/angiotensin/aldosterone system, besides leptin and adipocin may play an important role in the physiopathology of renal dysfunction in obese patients [10-12]. One can observe increase renal sodium reabsorption, besides the recruitment of functional reserve with glomerular hyper filtration. Obesity can also promote hypo filtration, increasing the risk for CKD [13-17].
Aiming to reduce the risk of obesity and its morbidities, as well as improving life quality of these individuals several clinical and surgical approach have been used including change in life style, drugs and surgical interventions [18]. Bariatric surgery has become the main operative way of controlling the associated morbidities, and an effective method for achieving sustained weight loss, improves blood pressure, reducing hyperglycemia, and even inducing diabetes remission [19-22].
The effect of bariatric surgery regarding the renal function is a subject of intensive research. In some papers [23-27] one can observe, after this operative procedure, improvement of glomerular filtration rate (GFR), reduction of hyper filtration and decrease in the micro albuminuria, preventing the onset of CKD and its progression. But in others, the improvement of kidney function is not well clear [28,29].
The purpose of this study was to evaluate the impact of bariatric surgery on renal function of the patients using a more sensitive biological marker such as cystatin C.
An observational, longitudinal and analytical study (cohort) was performed, in the Obesity Department from Campina Grande – Paraiba, Brazil. The investigation was approved by the Ethics Committee of the Faculty of Medical Sciences - UNIFACISA - Campina Grande – Paraíba, Brazil. All patients who participated in the study signed the informed consent form.
The criteria for performing bariatric surgery followed the recommendation of the National Consensus of Health Institutes with body mass index (BMI) ≥ 40kg/m2 without comorbidities or ≥ 35kg/m2 associated with comorbidities [30]. BMI was obtained by weight, in kilograms, divided by height, by squared meter, and classified according to the protocol established by the World Health Organization (WHO) [31].
The sample was of convenience, being recruited 35 patients who underwent bariatric surgery (12 bypass and 23 sleeve) with follow-up of at least one year, with ages from 24 to 57 years of age. Those with thyroid disease and with microalbuminuria ≥ 30mg/g were excluded to avoid patients with the possibility of already having diabetes mellitus nephropathy and/or systemic arterial hypertension.
The weight was measured using a calibrated digital body scale Tanita BC533®, because it is more resistant, with the patient standing in barefoot, with light clothes, without props. Height was measured by a stadiometer, with the subject standing, barefoot, with heels together, back straight and arms extended at the side of the body.
Blood samples were collected in the morning after a fasting period of at least 12 hours.
The creatinine dosage was performed from the isotope dilution mass spectrometry (IDMS) methodology, according with organizations involved with laboratory quality management programs, for monitoring of total analytical error linked to the method, with a result expressed in mg/dL [32].
The cystatin C was measured by nephelometry and later calibrated to recent cystatin C standardization, with a result expressed in mg/L [33].
The estimated glomerular filtration rate (GFR) was calculated using Nefrocalc 2.0 through the CKD-EPi creatinine- cystatin C equation. After the calculation of the GFR, a correction was made for the corresponding body surface [34]. It was defined normal GFR between 90 and 120 mL/min/1.73 m2, hypo filtration was defined by GFR < 90> 120mL/min/1.73 m2 [23].
The adjustment for body surface was made as follows: [23]
The samples were gathered from the obesity out patient department when they were coming for the preoperative period and at least one-year post-operative follow-up.
The sample was of convenience. Quantitative variables were expressed by the mean and standard deviation. Paired tests were used for assessing difference between means. Chi square test and exact Fisher were used for difference among frequencies. p ≤ 0.05 was used for rejecting the null hypothesis.
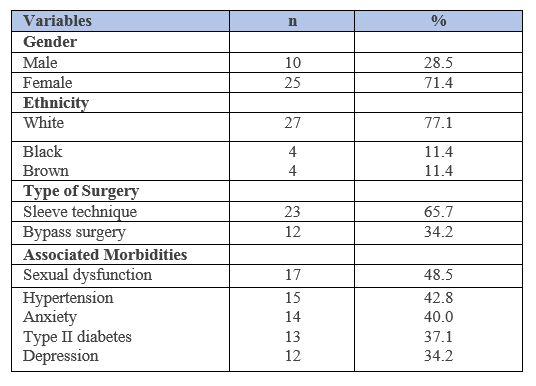
Twenty-five women (71.4%) and 10 man (28.5%) were randomly recruited for the research. Among them, 27 (77.1%) were white, four black (11. 4%) and four brown (11.4%). The mean age of them was 41.4 ± 9.7 years ranging from 24.0 to 57.0 years; the median was 42.0 years.
The more frequent associated morbidities were: sexual dysfunction (n = 17 – 48.5%); hypertension (n =15 – 42.8%): type II diabetes (n =13 – 37.1%); anxiety (n = 14 – 40.0%); and depression (n = 12 – 34.2%). Twenty-three (65.7%) patients underwent sleeve technique and 12 (34.2%) to bypass surgery. Table 1.
The mean time of follow-up was 16.2 ± 2.6 months ranging from 12 to 22 months; median 18 months.
It was observed a significant reduction of BMI in the post-operative follow-up (pre-operative: mean 40.3 ± 5.7 versus post-operative: mean 29.5 ± 4.5 – p < 0 xss=removed>
Among the patients with hypertension the majority (12 out of 15 – 80.0%) obtained control without medication and three (20%) required medication for controlling their blood pressure.
Among the diabetic patients, 10 (76.9%) obtained control of this morbidity. However, three (23.1%) remained with the need of medication for control of this morbidity.
Regarding sexual dysfunction, 14 (82.3%) patients obtained improvement of this construct and three (17.6%) remained the same status. Furthermore, eight out of 12 (66.6%) informed better control of depression and five (35.7%) out of 14 decrease their anxiety.
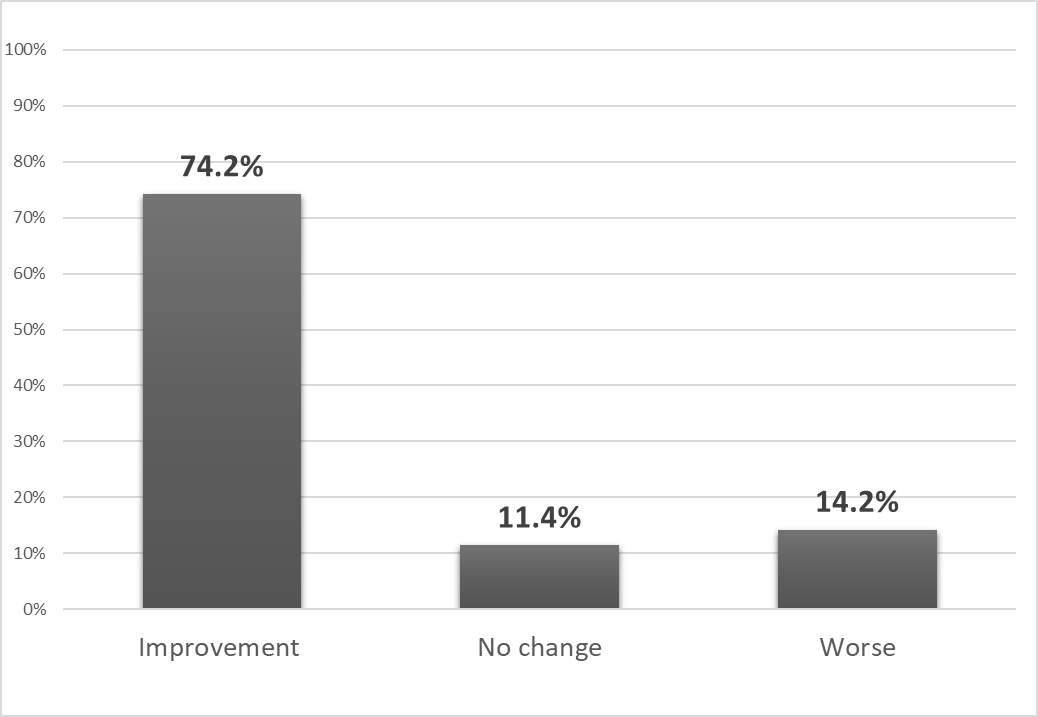
It was observed a significant improvement of glomerular filtration rates of obese patients who underwent bariatric surgery (preoperative 91.9 ± 17.8mL/min/1.73m2 ranging from 50.9 to 132.3 mL/min/1.73 m2- median of 90.8 mL/min/1.73 m2 versus - follow up - 100.5 ± 14.3 mL/min/1.73 m2, ranging from 62.7 to 129.8 mL/min/1.73 m2 - with a median of 100.6 mL/min/1.73 m2 – p = 0.0091). Out of 35 recruited patients, 26 (74.2%) improved GFR, four (11.4%) did not change GFR and five (14.2%) worsened GFR. Figure 1.
The improvement of renal function was more significant among those who underwent sleeve surgery as compared to bypass (22 out of 23 – 95.6% versus 5 out of 12 – 41.6% - p = 0.0008).
Obesity, as human being earth problem, has been continually increasing its prevalence, as well as its associated comorbidities and health care costs. Effective management of obesity and early intervention measures are necessary to overcome this global issue. The responsibility for preventing and managing this global epidemic does not lie solely on an individual, but also on the entire society and the health care systems [2,4].
Multidisciplinary approaches for obesity management and the collaboration among clinical physicians, endocrinologists, nutritional professionals, physiotherapists, psychiatrists, surgeons and nurses need to be improved across the whole globe to tackle this huge health issue, which great affect the life quality [1].
Bariatric surgery remains the best strategy for the management of obesity regarding to effective and sustained weight loss. One can observe, in this study, a significant weight lost after at least one year follow-up of these patients, as indicated in several studies [18-22, 35].
As regard to comorbidities (hypertension and diabetes) one can observe significantly decrease of the prevalence of these diseases after bariatric surgery, similar to most studies [18-22,36]. Similarly, there was improvement of sexual dysfunction, especially among those who could control anxiety and depression [37].
Cystatin C has been used as biological marker for renal function due to its high sensitivity and specificity and it is not influenced by weight loss [23, 38-40], reasoning because it was used for assessing renal function after bariatric surgery in obese patients in the present study. Hyperthyroidism has been shown to increase and hypothyroidism to decrease cystatin C serum concentrations, reasoning because thyroid disease was excluded [41].
Cystatin C has been used, successfully, for assessing renal function in child and adolescents obese. However, there was no difference between this metabolic parameter, when compared obese and non-obese individuals [42].
Studies have pointed the improvement of renal function after bariatric surgery, either with increased glomerular filtration rate in patients with chronic kidney disease, or reduction of hyper filtration in patients with no evidence of kidney disease. In this regard, the present results give support to this evidence, which can be summarized in improvement of renal function after bariatric surgery [27, 34, 43-46]
There are also renal risks in bariatric surgery, namely, acute kidney injury, nephrolithiasis, and, in rare cases, oxalate nephropathy, particularly in types of surgery involving higher degrees of malabsorption. Although bariatric surgery may improve long-term kidney outcomes, this potential benefit remains unproved and must be balanced with potential adverse events [47]
Renal function improvement was more evident among the patients who underwent sleeve technique. However, whether any kind of bariatric surgery delays the deterioration progression of this crucial biological function is still debatable subject. Large randomized prospective studies with a longer follow-up are needed [27].
Recent data, in obese adolescents, indicate that patients who require bariatric surgery may need a more personal technique as part of medicine precision for protecting kidney function, especially when long term outcome is anticipated. Furthermore, future non-surgical interventions therapies may mitigate the morbidities associated with obesity [25].
First, the sample size is too small for definitive evidence on this important question. Second, the follow-up time could not be sufficient for assessing renal function after bariatric surgery in obese patients. On the other hand, cystatin C has been used for assessing renal function in children and adolescents, but not in adults as it is in this investigation. Even though, the study has made a contribution for this challenging and unsolved question–Does bariatric surgery improve kidney function?
Significant improvement of glomerular filtration rate was observed, when compared the pre- and post-bariatric surgery periods, corroborating other studies that came to the same results. Furthermore, this outcome is more evident among patients who underwent sleeve technique. Further larger and longer post-operative follow-up cohorts are required for better answer of the main purpose of this health issue.
BMI: body mass index; GFR: glomerular filtration rate; CKD: chronic kidney disease; CKD-EPi: Chronic Kidney Disease Epidemiology collaboration; WHO: World Health Organization; IDMS: isotope dilution mass spectrometry; BSA: body superficial area; mGFR: measured glomerular filtration rate; eGFR: estimated glomerular filtration rate.
Ethics approval and consent to participate
The Institutional Ethical Committee of Faculty of Medicine –Campina Grande – Paraiba, Brazil approved the research under the number- 79501417.0.0000.5175.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests
Funding
The first author funded the research.
Authors' contributions
Bezerra JAB: collected the data, contributed in interpretation of data and prepared the manuscript.
Brandt CT: contributed in interpretation of data and made the final revision.
Borborema DMB: collected the data.
Dal Monte GBL: collected the data.
Maciel FAMF: contributed in interpretation of data.
Acknowledgements
Not applicable.
Authors' information
This manuscript is part of an ongoing thesis for obtained the PhD in surgery, from the Federal University of Pernambuco.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
