
Research Article | DOI: https://doi.org/10.31579/2693-7247/055
1 M. Pharm., Ph. D, Associate Professor, Department of Pharmaceutics, Unity College of Pharmacy, Telangana, India.
2 B. Pharm, Unity College of Pharmacy, Telangana, India.
*Corresponding Author: G. Prasad M. Pharm., Ph. D, Associate Professor, Department of Pharmaceutics, Unity College of Pharmacy, Telangana, India.
Citation: G. Prasad, K. Devika, P. Varshith, B. Shravani, E. Pavithra and Ch. Swathi (2021) Design and Optimizations of Aceclofenac Bioadhesive Extended Release Microspheres Development; J. Pharmaceutics and Pharmacology Research 4(4) DOI: 10.31579/2693-7247/055
Copyright: © 2021, G. Prasad, This is an open access article distributed under the Creative Commons Attribution License, which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 October 2021 | Accepted: 02 November 2021 | Published: 13 November 2021
Keywords: microspheres; zaltoprofen; aceclofenac
The oral route for drug delivery is the most popular, desirable, and most preferred method for administrating therapeutically agents for systemic effects because it is a natural, convenient, and cost effective to manufacturing process. Oral route is the most commonly used route for drug administration. Although different route of administration are used for the delivery of drugs, oral route remain the preferred mode. Even for sustained release systems the oral route of administration has been investigated the most because of flexibility in designing dosage forms.
Present controlled release drug delivery systems are for a maximum of 12 hours clinical effectiveness. Such systems are primarily used for the drugs with short elimination half life.
For many decades, medication of an acute disease or a chronic disease has been accomplished by delivering drugs to the patients via various pharmaceutical dosage forms like tablets, capsules, pills, creams, ointments, liquids, aerosols, injectable and suppositories as carriers [1]. To achieve and then to maintain the concentration of drug administered within the therapeutically effective range needed for medication, it is often necessary to take this type of drug delivery systems several times in a day. This results in a fluctuated drug level and consequently undesirable toxicity and poor efficiency. This factor as well as other factors such as repetitive dosing and unpredictable absorption leads to the concept of controlled drug delivery systems [2, 3]. The word new or novel in the relation to drug delivery system is a search for something out of necessity. An appropriately designed sustained or controlled release drug delivery system can be major advance toward solving the problem associated with the existing drug delivery system.
The objective of controlled release drug delivery includes two important aspects namely spatial placement and temporal delivery of drug. Spatial placement relates to targeting a drug to a specific organ or tissue, while temporal delivery refers to controlling the rate of drug delivery to the target tissue.
Oral controlled release dosage forms have been developed over the past three decades due to their considerable therapeutic advantages such as ease of administration, patient compliance and flexibility in formulation. However, this approach is be filled with several physiological difficulties such as inability to restrain and locate the controlled drug delivery system within the desired region of the gastrointestinal tract (GIT) due to variable motility and relatively brief gastric emptying time (GET) in humans which normally averages 2-3 h through the major absorption zone, i.e., stomach and upper part of the intestine can result in incomplete drug release from the drug delivery system leading to reduced efficacy of the administered dose.
The objective in designing a controlled release system is to deliver the drug at a rate necessary to achieve and maintain a constant drug blood level. This rate should be similar to that achieved by continuous intravenous infusion where a drug is provided to the patient at a rate just equal to its rate of elimination. This implies that the rate of delivery must be independent of the amount of drug remaining in the dosage form and constant over time, i.e., release from the dosage form should follow zero-order kinetics.
Preformulation Studies
Spectroscopic Studies
Preparation of 0.1N HCl (pH 1.2)
Take 8ml of HCl in a 1000ml volumetric flask and make up the volume with distilled water
Determination of λMax:
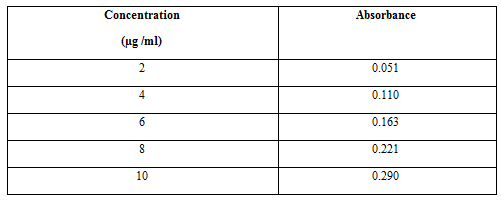
Stock solution (1000µg/ml) of Aceclofenac was prepared in methanol. This solution was appropriately diluted with 0.1N HCl(pH 1.2) and 6.8 pH phosphate buffer to obtain a concentration of 10µg/ ml. The resultant solution was scanned in the range of 200nm to 400nm on UV-Visible spectrophotometer. The drug exhibited a λmax at 252nm and 254nm.
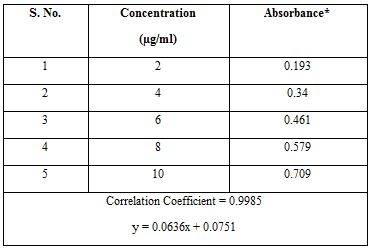
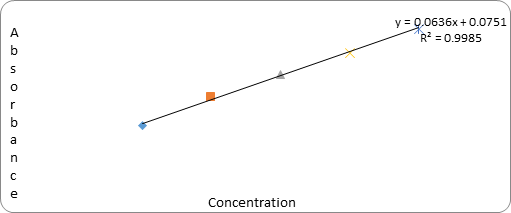
Preparation of Standard Calibration Curve of Aceclofenac:
The Linear Regression Analysis:
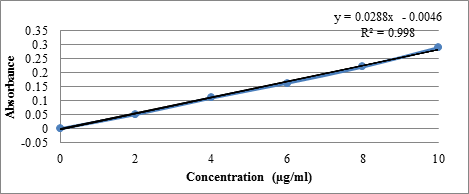
The linear regression analysis was done on Absorance points. The standardcalibration curve obtained had a Correlation Coefficient of 0.998 with of slope of 0.028 and intercept of 0.004.
Compatibility Studies
A proper design and formulation of a dosage form requires considerations of the physical, chemical and biological characteristics of both drug and excipients used in fabrication of the product. Compatibility must be established between the active ingredient and other excipients to produce a stable, efficacious, attractive and safe product. If the excipient(s) are new and if no previous literature regarding the use of that particular excipient with an active ingredient is available, then compatibility studies are of paramount importance. Hence, before producing the actual formulation, compatibility of Aceclofenac with different polymers and other excipients was tested using the Fourier Transform Infrared Spectroscopy (FT-IR) technique.
Fourier Transform Infrared Spectroscopy (Ft-Ir):
In order to check the integrity (Compatibility) of drug in the formulation,FT-IR spectra of the formulations along with the drug and other excipients were obtained and compared using Shimadzu FT-IR 8400 spectrophotometer. In the present study, Potassium bromide(KBr) pellet method was employed. The samples were thoroughly blended with dry powdered potassium bromide crystals. The mixture was compressed to form a disc. The disc was placed in the spectrophotometer and the spectrum was recorded.The FT-IR spectra of the formulations were compared with the FT-IR spectra of the pure drug and the polymers.
Ionotropic Gelation Method:
Batches of microcapsules were prepared by ionotropic gelation method which involved reaction between sodium alginate and polycationic ions like calcium to produce a hydrogel network of calcium alginate. Sodium alginate and the mucoadhesive polymer were dispersed in purified water (10 ml) to form a homogeneous polymer mixture. The API, Aceclofenac (100 mg) were added to the polymer premix and mixed thoroughly with a stirrer to form a viscous dispersion. The resulting dispersion was then added through a 22G needle into calcium chloride (4% w/v) solution. The addition was done with continuous stirring at 200rpm. The added droplets were retained in the calcium chloride solution for 30 minutes to complete the curing reaction and to produce rigid spherical microcapsules. The microcapsules were collected by decantation, and the product thus separated was washed repeatedly with purified water to remove excess calcium impurity deposited on the surface of microcapsules and then air-dried.

Characterization of Microcapsules:
Percentageyield
The percentage of production yield was calculated from the weight of dried microsphe-res recovered from each batch and the sum of the initial weight of starting materials. The percentage yield was calculated using the following formula:
Practical mass (Microcapsules)
% Yield=-----------------------------------------------x100
Theoretical mass (Polymer + Drug)
Drug entrapment efficiency:
Microcapsules equivalent to 100 mg of the drug Aceclofenac were taken for evaluation. The amount of drug entrapped was estimated by crushing the microcapsules. The powder was transferred to a 100 ml volumetric flask and dissolved in 10ml of methanol and the volume was made up using simulated gastric fluid pH 1.2. After 24 hours the solution was filtered through Whatmann filter paper and the absorbance was measured after suitable dilution spectrophotometrically at 252 nm. The amount of drug entrapped in the microcapsules was calculated by the following formula,
Experimental Drug Content
% Drug Entrapment Efficiency = - - - - - - - - - - - - - - - - - - - - - - - × 100
Theoretical Drug Content
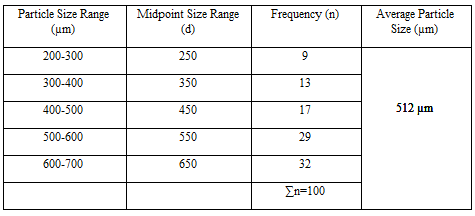
Particle size analysis:
Samples of the microparticles were analyzed for particle size by optical microscope. The instrument was calibrated and found that 1unit of eyepiece micrometer was equal to 12.5μm. Nearly about 100 Microparticles sizes were calculated under 45x magnification. The average particle size was determined by using the Edmondson’s equation:
nd
Dmean=------
n
Where,
n – Number of microcapsules observed
D – Mean size range
Swelling study:
Swelling ratio of different dried microcapsules were determined gravimetrically in simulated gastric fluid pH 1.2 .The microcapsules were removed periodically from the solution, blotted to remove excess surface liquid and weighed on balance. Swelling ratio (% w/v) was determined from the following relationship:
(Wt – W0)
Swelling ratio = - - - - - - - - - - - × 100
(W0)
Where W0 & Wt are initial weight and Final weight of microcapsules respectively.
Evaluation of mucoadhesive property:
The mucoadhesive property of microcapsules was evaluated by an in vitro adhesion testing method known as wash-off method. Freshly excised pieces of goat stomach mucous were mounted on to glass slides with cotton thread. About 20 microcapsules were spread on to each prepared glass slide and immediately thereafter the slides were hung to USP II tablet disintegration test, when the test apparatus was operated, the sample is subjected to slow up and down movement in simulated gastric fluid pH 1.2 at 370C contained in a 1-litre vessel of the apparatus. At an interval of 1 hour up to 8 hours the machine is stopped and number of microcapsules still adhering to mucosal surface was counted.
Number of microcapsules adhered
% Mucoadhesion= ------------------------------------------ ×100
Number of microcapsules applied
In vitro drug release study:
The dissolution studies were performed in a fully calibrated eight station dissolution test apparatus (37 ± 0.50C, 50 rpm) using the USP type – I rotating basket method in simulated gastric fluid pH 1.2 (900ml). A quantity of accurately weighed microcapsules equivalent to 100mg Aceclofenac each formulation was employed in all dissolution studies. Aliquots of sample were withdrawn at predetermined intervals of time and analyzed for drug release by measuring the absorbance at 252nm. At the same time the volume withdrawn at each time intervals were replenished immediately with the same volume of fresh pre-warmed simulated gastric fluid pH 1.2 maintaining sink conditions throughout the experiment.
4.1. Preformulation Studies
4.1.1. Spectroscopic Studies
Determination of λmax
A solution of 10µg/ml of Aceclofenac was scanned in the range of 200 to 400nm. The drug exhibited a λmax at 252nm in simulated gastric fluid pH 1.2 and had good reproducibility. Correlation between the concentration and absorbance was found to be near to 0.998, with a slope of 0.028 and intercept of 0.004.
Calibration curve of Aceclofenac in simulated gastric fluid pH 1.2
Compatibility Studies
Drug polymer compatibility studies were carried out using Fourier Transform Infra-Red spectroscopy to establish any possible interaction of Drug with the polymers used in the formulation. The FT-IR spectra of the formulation were compared with the FTIR spectra of the pure drug.
Evaluation and Characterisation of Microspheres
Percentage Yield
It was observed that as the polymer ratio in the formulation increases, the product yield also increases. The low percentage yield in some formulations may be due to blocking of needle and wastage of the drug- polymer solution, adhesion of polymer solution to the magnetic bead and microspheres lost during the washing process. The percentage yield was found to be in the range of 80 to 88% for microspheres containing sodium alginate along with GUAR GUMas copolymer, 62.22 to 87% for microspheres containing sodium alginate along with LOCUST BEAN GUM as copolymer and 80 to 87.5% for microspheres containing sodium alginate along with XANTHAN GUMas copolymer. The percentage yield of the prepared microspheres is recorded in Table 6.2 and displayed in Figures 6.4 to 6.6.
Drug Entrapment Efficiency
Percentage Drug entrapment efficiency of Aceclofenac ranged from 82.66 to 88.66% for microspheres containing sodium alginate along with GUAR GUMas copolymer, 53.2 to 76.66% for microspheres containing sodium alginate along with Locust Bean Gum as copolymer and 66.73 to 79.2% for microspheres containing sodium alginate along with Xanthan Gum as copolymer. The drug entrapment efficiency of the prepared microspheres increased progressively with an increase in proportion of the respective polymers. Increase in the polymer concentration increases the viscosity of the dispersed phase. The particle size increases expone- ntially with viscosity. The higher viscosity of the polymer solution at the highest polymer concentration would be expected to decrease the diffusion of the drug into the external phase which would result in higher entrapment efficiency. The % drug entrapment efficiency of the prepared microspheres is displayed in Table 6.3, and displayed in Figures.

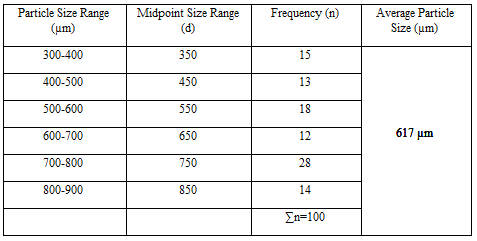
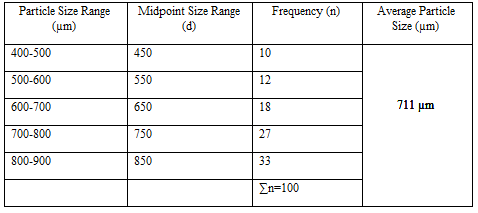
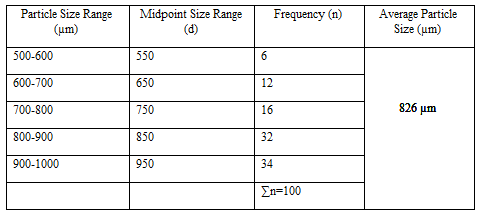
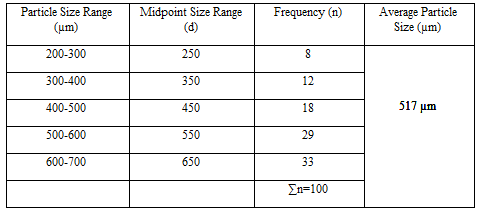
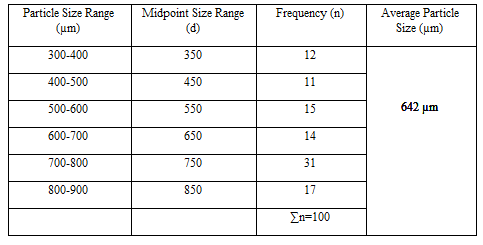
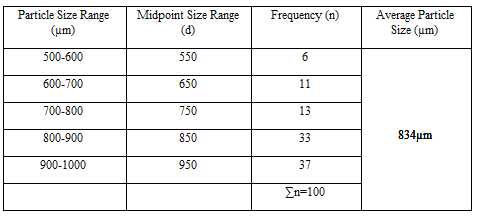
Particle Size Analysis
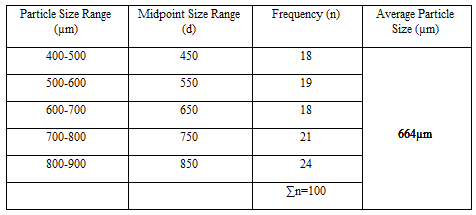
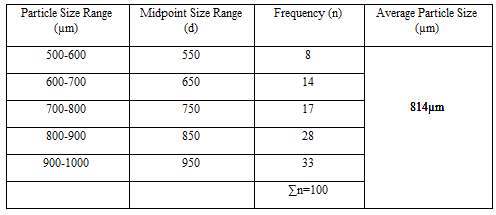
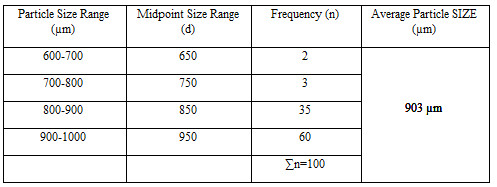
The mean size increased with increasing polymer concentration which is due to a significant increase in the viscosity, thus leading to an increased droplet size and finally a higher microspheres size. Microspheres containing sodium alginate along with Guar gum as copolymer had a size range of 512µm to 826µm, microspheres containing sodium alginate along with Locust Bean Gum as copolymer exhibited a size range between 517µm to 834µm and microspheres containing sodium alginate along with XANTHAN GUM as copolymer had a size range of 664µm to 903µm. The particle size data is presented in Tables 6.3 to 6.13 and displayed in Figures. The effect of drug to polymer ratio on particle size is displayed in Figure. The particle size as well as % drug entrapment efficiency of the microspheres increased with increase in the polymer concentration.


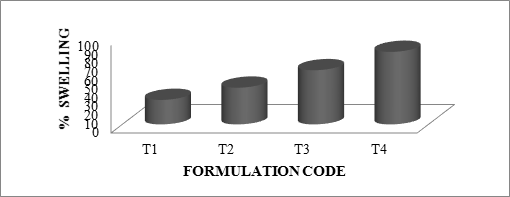
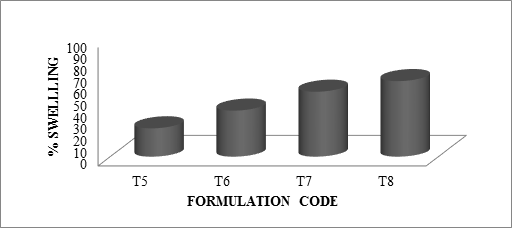
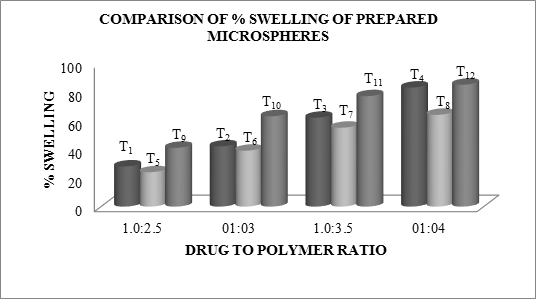
The swelling ratio is expressed as the percentage of water in the hydrogel at any instant during swelling. Swell ability is an important characteristic as it affects mucoadhesion as well as drug release profiles of polymeric drug delivery systems. Swell ability is an indicative parameter for rapid availability of drug solution for diffusion with greater flux. Swell ability data revealed that amount of polymer plays an important role in solvent transfer. It can be concluded from the data shown in Table 6.14 that with an increase in polymer concentration, the percentage of swelling also increases. Thus we can say that amount of polymer directly affects the swelling ratio. As the polymer to drug ratio increased, the percentage of swelling increased from 28 to 85% for microspheres containing sodium alginate along with GUAR Gum as copolymer, 24 to 64% for microspheres containing sodium alginate along with Locust Bean Gum as copolymer and 31 to 85 for microspheres containing sodium alginate along with Xanthan Gum as copolymer. The percentage of swelling of the prepared microspheres is displayed in Figures. The effect of drug to polymer ratio on percentage swelling is displayed in Figure.


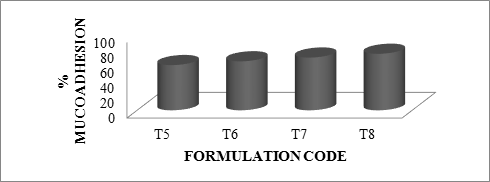
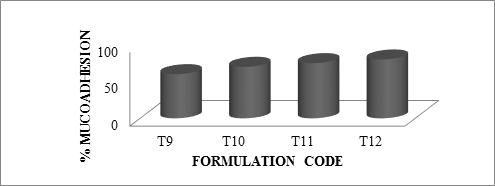
In-Vitro Mucoadhesion Test
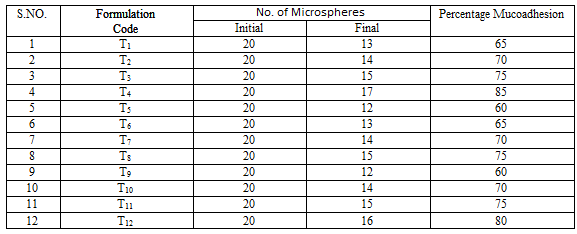
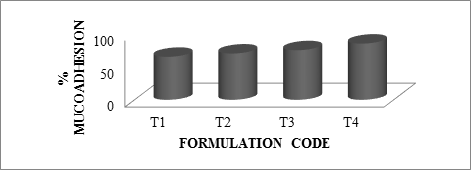
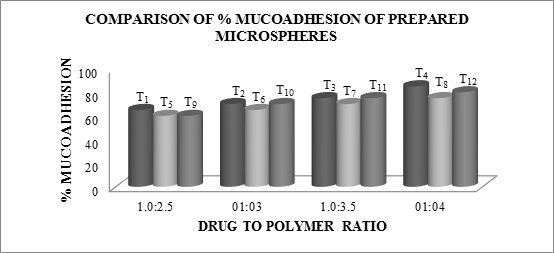
As the polymer to drug ratio increased, microspheres containing sodium alginate along with Guar Gum as copolymer exhibited % mucoadhesion ranging from 65 to 85%, microspheres containing sodium alginate along with Locust Bean Gum as copolymer exhibited % mucoadhesion ranging from 60 to 75% and microspheres containing sodium alginate along with Xanthan Gum as copolymer exhibited % mucoadhesion ranging from 60 to 80%.
The rank of order of mucoadhesion is Guar Gum> Xanthan Gum > Locust Bean Gum. The results of in-vitro mucoadhesion test are compiled in Table 6.15. Effect of polymer proportion on % mucoadhesion is depicted in Figures 6.14 to 6.16 and comparative depiction of % mucoadhesion is depicted in Figure 6.17.
In-Vitro Drug Release Studies
Dissolution studies of all the formulations were carried out using dissolution apparatus USP type I. The dissolution studies were conducted by using dissolution media, pH 1.2.for fisrt 2hr and then it was eplaced with 6.8ph phosphate buffer The results of the in-vitro dissolution studies of formulations T1 to T4, T5 to T8 and T9 to T12 are shown in table. The plots of Cumulative percentage drug release Vs Time. Figure shows the comparison of
In thepresent work, bioadhesive controlled release microspheresof Zaltoprofen using Sodium alginate along with HPMC K100M, HPMC K15M, XANTHAN GUMas copolymers wereformulated to deliver Zaltoprofen via oral route.
Details regarding the preparation and evaluation of the formulations have been discussed in the previous chapter. From the study following conclusions could be drawn:-
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
