
Case Report | DOI: https://doi.org/10.31579/2690-1919/166
*Corresponding Author: Marilena Stoian, University of Medicine and Pharmacy “Carol Davila”, Bucharest, Romania.
Citation: Marilena Stoian (2021). Clostridium Difficile Infection and Biliary Obstruction. J Clinical Research and Reports, 8(1); DOI:10.31579/2690-1919/166
Copyright: © 2021 Marilena Stoian, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 May 2021 | Accepted: 17 May 2021 | Published: 31 May 2021
Keywords: crohn disease; endoscopic retrograde cholangiopancreatography; primary sclerosing cholangitis; clostridium difficile infection; metronidazole; ultrasonographic examination
We present a case of a 38-year -old man was admitted to the hospital with biliary obstruction and Clostridium Difficile infection. He presented with moderate increases in the aminotransferase and bilirubin levels suggesting the diagnosis of an autoimmune hepatobiliary disease; intestinal protein loss needs to evaluate an associated inflammatory bowel disease. The clinical diagnosis of autoimmune hepatobiliary disease associated with inflammatory bowel disease is based on the patients symptoms and the presence of a protein-losing enteropathy which are more suggestive of Crohn disease, while moderate increases in the aminotransferase levels in proportion to the increase in the bilirubin level suggesting the diagnosis of primary sclerosing cholangitis. The pathological and positive diagnosis needs an endoscopic retrograde cholangiopancreatography and a biopsy of gastric and duodenum mucosae who showed severe inflammation findings that are diagnostic of Crohn disease.
Case Report:
A 38-year -old man was admitted to the hospital because of evidence of biliary obstruction and 3 kg lost in weight during the last two weeks. One year before admission, the patient was admitted to another hospital because of bloody diarrhea, when the serum aspartate aminotransferase level was 100 U per liter and a test for Clostridium Difficile was positive. He had not taken antibiotics before the onset of symptoms and it was prescribed one- month of metronidazole. The patient condition was well until several weeks before admission, when he began to have no radiating colicky pain in the epigastrium, right upper quadrant, and periumbilical area; the pain was exacerbated by eating and was accompanied by nausea. He also began to have intermittent loose stools without frequent or voluminous diarrhea. During the two weeks before admission, his temperature rose intermittently to 38.30 C. Five days before admission, the patient had left-sided pleuritic chest pain and a dry cough. He went to another hospital, where leukocytosis with a left-ward shift was found. Findings on a radiograph of the chest suggested the presence of pneumonia of the right lower lobe; there was bilateral prominence of the interstitial markings. An abdominal ultrasonographic examination revealed no abnormalities and because the pain was constantly and the no medication effective the patient was transferred to our hospital.
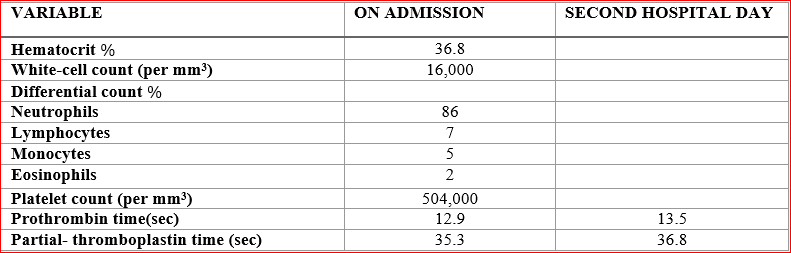
The patient was an advocate with no history of the use of alcohol and no family history of inflammatory bowel disease or rheumatic disorders. The temperature was 37.80 C, the pulse was 85, the respiration rate was 20, and the blood pressure was 120/55mm/Hg. Physical examination revealed mild scleral icterus and market tenderness over the sternum on palpation, with abdomen soft with slight tenderness in the right upper quadrant; there was no hepatomegaly. No protozoa or helminthic ova were found on microscopical examination of the stool; assay of a stool culture yielded no enteric pathogens. The urine was positive for bile and for urobilinogen. Laboratory test were performed (Tables 1, 2, 3).


Radiographs of the chest revealed bilateral prominence of the interstitial markings. An ultrasonographic examination of the abdomen showed that the liver had a normal texture and the intrahepatic ducts and the common bile duct were of normal diameter. The gallbladder was partially collapsed; the pancreas appeared normal. Ranitidine, Cephotaxime and Acetaminophen were given, but the patient s temperature rose into the evening to 39.70 C. On the second hospital day, the patient s temperature did not exceed 390 C and the abdominal pain had ceased. A computed tomographic (CT) examination of the abdomen and pelvis performed after the oral and intravenous administration of contrast material, revealed no abnormalities.
A stool test for Clostridium Difficile toxin was positive at that time and although the illness responded to metronidazole, community-acquired Clostridium Difficile -related disease would be unusual in a young man, particularly in the absence of known predisposing factors. Only 1 to 3 percent of adults are healthy carriers of Clostridium Difficile [1, 2]. The most common risk factors for the acquisition of clinical Clostridium Difficile -related disease are hospitalization and the use of antibiotics; other risk factors include advanced age, previous nonsurgical gastrointestinal procedures, an immunocompromised state, and the presence of underlying factors [3, 4]. However, it was reported that Clostridium Difficile infection may be associated with a relapse of symptoms in patients with inflammatory bowel disease, in whom this infection can occur even in the absence of antibiotic use [5]. In our case metronidazole was given for one month, which is longer than the recommended length of treatment for an uncomplicated Clostridium Difficile infection [6, 7].
During the initial illness, the patient also had a slightly elevated aspartate aminotransferase level, a finding that is not usually associated with Clostridium Difficile infection and that could be explained by a variety of acute or chronic diseases; most of them can rules out by his subsequent clinical course and the results of his laboratory tests.
The differential diagnosis in this case should focus on clinical disorders that can cause intestinal disease as well as hepatobiliary disease. (Figure 1) The two major diseases or categories of disease than can explain this patient s intestinal disorder are celiac sprue and inflammatory bowel disease.

Celiac sprue is a well-recognized cause of enteric loss of protein and enteric malabsorption. There is a documented association between celiac sprue and autoimmune liver diseases, including autoimmune hepatitis, primary biliary cirrhosis, and primary sclerosing cholangitis [8-20]. Nonspecific elevations in aminotransferase levels are common and usually resolve with a gluten-free diet. Celiac sprue is an unlikely diagnosis in the current case, because this illness generally develops in adults or in children who are younger than this patient. In addition, an acute onset of marked upper gastrointestinal symptoms is atypical of celiac disease, although in this case such symptoms could be related to the liver disease.
Our patient s illness is most consistent with the diagnosis of inflammatory bowel disease. Both ulcerative colitis and Crohn s disease are associated with intestinal protein loss and hepatobiliary disorders, including autoimmune diseases [21-24]. The initial signs, symptoms, and laboratory findings that suggest inflammatory bowel disease include diarrhea, fever, wight loss, leukocytosis, thrombocytosis, and occult blood in the stool. The patient s substernal pain may have been due to esophageal involvement. Upper gastrointestinal involvement is more common in children with inflammatory bowel disease than in adults. In one series, 80 percent of patients with Crohn s disease and 75 percent of those with ulcerative colitis had endoscopic abnormalities such as esophagitis, gastritis, duodenitis, and upper gastrointestinal ulcers [25, 26].
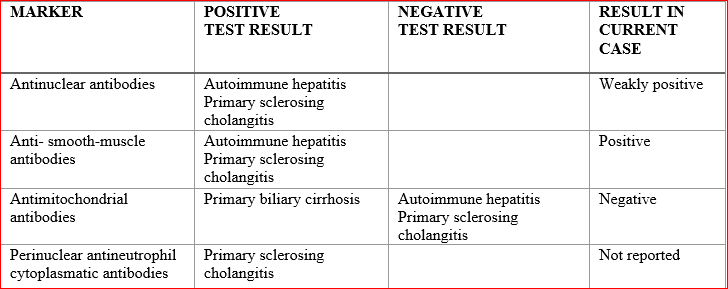
The findings on radiographic and laboratory evaluation of the patient s hepatobiliary disease eliminate a number of disorders from differential diagnosis. Abdominal CT and ultrasonographic studies did not reveal evidence of stones, gallbladder disease, or biliary tract dilatation, and the liver appeared to have a normal texture. Autoimmune liver diseases are common in both ulcerative colitis and Crohn s disease. On the other hand, both primary sclerosing cholangitis and autoimmune hepatitis also occur in association with inflammatory bowel disease. Sclerosing cholangitis can involve the extrahepatic ducts, the intrahepatic ducts, or both. The frequency of this disorder in patients with inflammatory bowel disease is about 10 percent [24]. Autoimmune hepatitis characteristically involves the hepatic parenchyma, although there are variant overlap syndromes with features of both autoimmune hepatitis and primary sclerosing cholangitis. These disorders can be differentiated by endoscopic retrograde cholangiopancreatography, evaluation of autoimmune markers, and liver biopsy. In our case, the results of marker studies are inconclusive, but a test for perinuclear antineutrophil cytoplasmatic antibodies might have been diagnostically helpful (Table 4).
The clinical diagnosis of autoimmune hepatobiliary disease associated with inflammatory bowel disease is based on the patients symptoms and the presence of a protein-losing enteropathy which are more suggestive of Crohn disease, while moderate increases in the aminotransferase levels in proportion to the increase in the bilirubin level suggesting the diagnosis of primary sclerosing cholangitis.
For the pathological diagnosis the first diagnostic procedure proposed was a liver biopsy, but the insufficiency of technical resources and no positive patient s accord for this procedure we performed an endoscopic retrograde cholangiopancreatographic study. It was ruled out obstruction of the extrahepatic bile ducts, a condition that can be associated with hepatic changes similar to those of primary sclerosing cholangitis. Examination of the both gastric fundus (Figure 2) and the duodenum (Figure 3) showed severe inflammation and an epithelioid granuloma in the gastric wall; there was patchy, superficial inflammation as well as deep acute and chronic inflammation. All of these findings are diagnostic of Crohn disease.


We decided to begin treatmentwith ursodiol (300 mg twice daily) and prednisone (20 mg daily), treatment administrated for 4weeks since the biochemical values return to normal, except for 5- nucleotidase value, which remained slightly elevated. The dose of prednisone was tapered during 6 months until discontinued and replaced with mesalamine. Thirty-six months after the diagnoses were made, the patient s aminotransferase levels were still slightly elevated, and his gamma-glutamyltransferase level was still moderate elevated. A repeat endoscopic retrograde cholangiopancreatogram showed no change in the degree of narrowing of the intrahepatic bile ducts. Once the synthetic function of the liver is sufficiently compromised, the only therapeutic option is transplantation. Ursodiol lowers the aminotransferase levels and improves the biochemical profile but does not affect the long-term outcome [27].
It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,

Dear Maria Emerson, Editorial Coordinator of International Journal of Clinical Case Reports and Reviews, What distinguishes International Journal of Clinical Case Report and Review is not only the scientific rigor of its publications, but the intellectual climate in which research is evaluated. The submission process is refreshingly free of unnecessary formal barriers and bureaucratic rituals that often complicate academic publishing without adding real value. The peer-review system is demanding yet constructive, guided by genuine scientific dialogue rather than hierarchical or authoritarian attitudes. Reviewers act as collaborators in improving the manuscript, not as gatekeepers imposing arbitrary standards. This journal offers a rare balance: high methodological standards combined with a respectful, transparent, and supportive editorial approach. In an era where publishing can feel more burdensome than research itself, this platform restores the original purpose of peer review — to refine ideas, not to obstruct them Prof. Perlat Kapisyzi, FCCP PULMONOLOGIST AND THORACIC IMAGING.
