
Case Report | DOI: https://doi.org/10.31579/2690-1919/167
1 Radiology Department, Usmanu Danfodiyo University, Sokoto
2 Radiology Department, Gombe State University, Gombe.
3 Radiology Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto
*Corresponding Author: SULE Muhammad Baba, Department of Radiology, Usmanu Danfodiyo University, Sokoto.
Citation: Sule MB, Shamaki AMB, Umar AU, Gele IH, Abdullahi A, et al (2021). Bilateral Protrusio Acetabuli in an Elderly Female Patient: The Plain Radiographic Features and a Case Report. J Clinical Research and Reports, 7(5); DOI:10.31579/2690-1919/167
Copyright: © 2021 SULE Muhammad Baba, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 04 May 2021 | Accepted: 11 May 2021 | Published: 17 May 2021
Keywords: plain radiograph; pelvic cavity; degenerative changes; acetabulum; arthroplasty; arthrokatadysis; femoroacetabular impingement
Protrusion acetabuli is the medial protrusion of the acetabulum in to the pelvic cavity, also known as arthrokatadysis, more common in females and classified etiologically as primary (idiopathic) and secondary forms.
This is a 66-year-old female patient that presented for a plain radiograph of the pelvis and hip joints from a peripheral healthcare center on account of pain and inability to stand and move her waist and hips bilaterally, reduced movement of the legs and pain in the knees for more than three-year duration of onset.
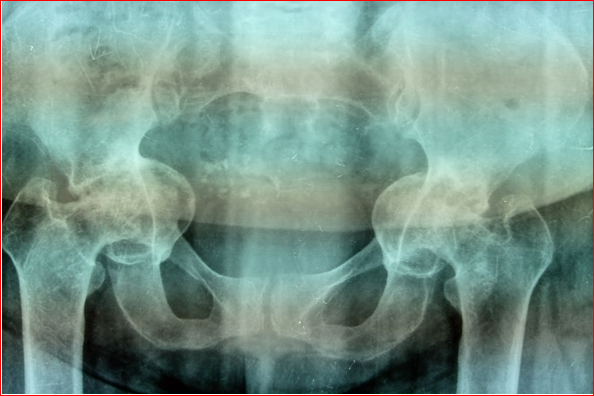
The plain radiograph of the pelvis and both hip joints demonstrate reduced density of the demonstrated bones, medial protrusion of the medial wall of the acetabulum in to the pelvic cavity bilaterally (distance between the imaginary Kohler’s line and medial acetabular wall is about 22mm bilaterally; Degree: III), obliteration of the hip joints bilaterally, thickening and sclerosis of the acetabular walls and other articular margins, subarticular cysts on the femur, acetabulum and pelvic bones. The patient had no coexisting condition like rheumatoid arthritis, Marfan’s syndrome and psoriatic arthritis. A diagnosis of bilateral idiopathic protrusio acetabuli was made. The patient was advised on bilateral total hip arthroplasty to improve the symptoms.
We report a case of bilateral idiopathic protrusion acetabuli in an elderly female patient in order to describe the features of this condition radiographically.
Protrusion acetabuli is defined as that condition associated with medial displacement of the femoral head into the pelvis, with the medial aspect of the femoral head lying medial to the ilioischial line[1,2].
Protrusio acetabuli (PA) could either be primary (idiopathic) and secondary forms, it could either be unilateral or bilateral affecting one or both hips, and could be bilateral in conditions like rheumatoid arthritis, Paget’s disease, ankylosing spondylitis, Marfan’s syndrome and osteomalacia [1,3].
Primary or idiopathic PA is often reserved in cases where no causative factors found, often regarded as a diagnosis of exclusion, while the secondary PA has an identifiable cause, with numerous conditions like neoplastic, inflammatory, metabolic, infectious, traumatic and genetic causes are implicated in the cause of PA [3].
The presence of bilateral involvement of the hips and in the female gender, with racial and hereditary influence has been described for primary PA [4-6].
In PA, forces acting on the hip depend on some contributors, these are body weight, distance from the center of the femoral head to the midline and femoral neck-shaft angle. These factors are predictable on the basis of Pauwels theories of hip biomechanics [3,7].
Acetabular protrusion causes displacement of the hip rotational center inwardly, thereby causing limb shortening, decreased gluteal muscle tension, and associated extreme hip pain which may lead to an impairment in daily activities of the patient often requiring total hip arthroplasty [8].
The pincer effect is regarded as an infrequent subtype of femoroacetabular impingement, and protrusion acetabuli is by large the most severe pincer form and has a global involvement, and requiring surgical dislocation with acetabular rim trimming [4,9].
Imaging play’s role in PA, the anterior-posterior and lateral views of plain radiographs of the pelvis, these are needed in making the diagnosis, staging the severity and monitoring the disease progression [1,3].
This is a 66-year-old female patient that presented for a plain radiograph of the pelvis and hip joints from a peripheral healthcare center on account of pain and inability to stand and move her waist and hips bilaterally, activity-related pains, reduced movement of the legs and pain in the knees for more than three-year duration of onset.
No family history of similar or related problems, the patient has no history of seropositive arthritis.
On examination, the patient is oriented and conscious, not pale, anicteric, not dehydrated, not in obvious respiratory distress, has antalgic gait with a positive Trendelenburg sign.
The blood pressure was about 120/75mmHg, pulse rate of about 72beats/minute, respiratory rate of about 12cycles per minute and non-elevated jugular vein.
The packed cell volume was 38%, white cell count of about 11000/m3 and an erythrocyte sedimentation rate of 8mm/hr. The blood electrolyte was normal, blood urea was normal (3.5mmol/L) and the blood creatinine was also normal (76mmol/L). The uric acid level and calcium levels were also normal (3.0milligrams per deciliter and 8.8milligrams per deciliter).
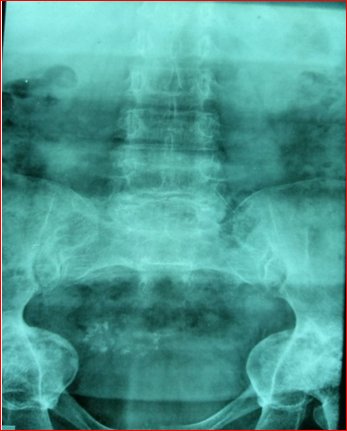
The plain radiograph of the pelvis and both hip joints; (anterior-posterior and left lateral views) demonstrate reduced density of the demonstrated bones, medial protrusion of the medial wall of the acetabulum in to the pelvic cavity bilaterally (distance between the imaginary Kohler’s line and medial acetabular wall is about 22mm bilaterally; Degree: III), obliteration of the hip joints bilaterally, thickening and sclerosis of the acetabular walls and other articular margins, subarticular cysts on the femur, acetabulum and pelvic bones (figure 1 and 2).

The anterior-posterior view of the lumbar spine showed degenerative changes involving the lumbar spine with no syndesmophytes (figure 3). The patient had no coexisting condition like rheumatoid arthritis, Marfan’s syndrome and psoriatic arthritis. A diagnosis of bilateral idiopathic protrusio acetabuli was made.
The patient was advised on bilateral total hip arthroplasty as the surgical treatment to improve the symptoms and improve quality of life, the patient however did not consent to this treatment option as at the time of this report.
Protrusion acetabuli was initially described in 1824 by Otto in cadaveric studies as a deformity of the medial wall of the acetabulum with associated migration of the femoral head in to the pelvis [10,11]. The case under review presented with features suggesting migration of both acetabulum in to the pelvic cavity medially in keeping with protrusion acetabuli, thereby conforming to this literature.
Protrusion acetabuli has a female preponderance with a ratio of about 10:1, and often bilateral more common in individuals with advanced rheumatoid arthritis [10,12]. The case under review happens to be a female with bilateral affectation of the hips, but not a case of rheumatoid arthritis, thereby conforming to these literatures.
Protrusion acetabuli has been classified as etiologically as either primary or idiopathic accounting for about 75.3% of cases and as secondary PA in about 24.7% of cases, and also classified radiologically as either mild, moderate and severe forms [10,13]. The index case is most likely the primary form since an etiology has not been established, and from the radiographic features, this resembles a severe form of PA, thereby conforming to these literatures.
Protrusion acetabuli has also been graded on plain pelvic radiograph as either Degree I: when the measurement from the medial aspect of the acetabulum and Kohler’s line is between 1-5mm (light protrusion), Degree II: when the measurement from the medial aspect of the acetabulum and Kohler’s line is between 6-15mm (mild protrusion), and Degree III: when the measurement from the medial aspect of the acetabulum and Kohler’s line is more than 15mm (severe protrusion) [10,13]. The index case is most likely in the Degree III category as an estimated measurement of the distance from the Kohler’s line from the acetabulum is about 22mm, thereby conforming to these literatures.
In making a diagnosis of PA, clinical history with adequate clinical examination and radiological imaging are vital, confirmation of the diagnosis is mainly by standard plain radiographs of the hips; the anterior-posterior and lateral views, these make diagnosis, stage the disease progression with severity [1,3,10,13]. The case under review was diagnosed following plain radiographs of the hips, thereby conforming to these literatures.
The mainstay of treatment in adults is surgery, patients with significant arthritis and PA need total hip arthroplasty (THA) with non-structural bone grafting of the medial wall cavity for effectiveness [1,3]. The case under review was also advised for THA, but as at the time of this report the patient is yet to consent to this treatment modality.
Protrusion acetabuli is a condition associated with severe painful episodes especially with movement of the hip joint, this could either be primary or secondary, and when suspected, plain anterior-posterior radiograph of the hip joint plays an important role in confirmation of the diagnosis and monitoring the disease and its severity.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
