AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2690-4861/364
1 Department of Epidemiological Surveillance Management, Hospital Dr. Francisco de Icaza Bustamante, Guayaquil, Ecuador.
2 Chair of Infectious Pathologies, Faculty of Medical Sciences, University of Guayaquil, Ecuador.
3 Responsible of the Dermatology Service, Kids Hospital "Dr. Francisco de Icaza Bustamante" Guayaquil, Ecuador.
4 Medical Specialist of Dermatology Service, Kids Hospital "Dr. Francisco de Icaza Bustamante" Guayaquil, Ecuador.
5 Faculty of Medical Sciences. University of Guayaquil, Ecuador.
*Corresponding Author: Velásquez Serra GC, Chair of Infectious Pathologies, Faculty of Medical Sciences, University of Guayaquil, Ecuador.
Citation: Caballero Pineda BX., Velásquez Serra GC., Zambrano Mora GC., Llanga Jairala LM., Sarango Bravo AL., et al., (2024), Bartonellosis (Oroya Fever, Peruvian Wart): A Case Report, International Journal of Clinical Case Reports and Reviews, 16(3); DOI:10.31579/2690-4861/364
Copyright: © 2024, Velásquez Serra GC. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 November 2023 | Accepted: 23 January 2024 | Published: 28 February 2024
Keywords: bartonella infections; medical records; vector borne diseases; Ecuador
Bartonellosis (also called Carrión's Disease, Oroya Fever or Peruvian Wart) is caused by the bite of mosquitoes of the Lutzomyia genus belonging to the Psychoid family. They are nocturnal blood-sucking insects, with complete metamorphosis. About 450 species are known, distributed throughout the American continent, mostly in tropical and subtropical areas. In Ecuador, sporadic cases have been reported, with certain characteristics such as, for example, not presenting the blood phase and, in the eruptive phase, not being aggressive. Here, we present a unique case of a 13-year-old boy with a history of congenital heart disease, who presented a clinical picture of one year of evolution suggestive of dermatosis, characterized by papules and nodules that occasionally bleed. The mother reports living in an area of lush vegetation and being in contact with bites. The results of blood count, peripheral blood smear, liver function and coagulation: normal. Blood sample: Negative Bartonella spp. PCR biopsy ribC gene: Positive B. bacilliformis. This case demonstrates the importance of maintaining an entomo-epidemiological surveillance system in patients exposed to arthropod bites that allows for timely detection of cases in order to make a diagnosis and provide timely treatment.
Human Bartonellosis is a biphasic bacterial infection caused by Bartonella bacilliformis. In 1993, American and European scientists found other species of bartonellae affecting humans and later others affecting only animals [1].
At the time of the Republic (1870-1906) a serious epidemic occurred during the construction of the Lima - La Oroya railroad (the highest in the world) in which thousands of workers (Chileans, Chinese, Bolivians, etc.) participated, of which more than 7,000 died, the disease being known as "Oroya Fever"; in some survivors appeared reddish dermal eruptions, which were given the name of Peruvian wart. This epidemic motivated great research interest in the international medical community [2].
The Peruvian medical student, Daniel Alcides Carrión, in 1885, investigated and established the clinical unity between Oroya fever and the Peruvian wart, thus becoming the martyr of Peruvian medicine. For this purpose, he inoculated the product of a verruca from a patient at the Hospital Dos de Mayo, in order to experiment in his own body, the development of the disease known as Peruvian wart [2,3].
In 1909, Alberto Barton, a medical microbiologist, discovered the etiological agent of Carrión's disease in the parasitized red blood cells of the anemic phase of the disease and described them as "end globular bodies", which was later catalogued as a bacterium identified with the name Bartonella bacilliformis in recognition of its discoverer [4].
Townsend, in 1913, identified the vector Lutzomyia verruca rum (popularly known as "titira" or "manta Blanca") as the transmitter of the disease, whose habitat is limited to the valleys of the Andean Mountain range of Colombia, Ecuador and Peru [3,4].
Lutzomyia’s are nocturnal hematophagous insects, with complete metamorphosis. About 450 species are known, distributed throughout the American continent, mainly in tropical and subtropical zones. The optimum temperature where they develop fluctuates between 19ºC - 23ºC; the average life span of the mosquito is 50 to 60 days [5].
Among the clinical manifestations, two phases are described: the acute, septicemic, febrile or anemic stage, known as Oroya fever, and the chronic, eruptive or Peruvian wart stage. It has an incubation period of 21 days (up to 7 months) [6].
The acute phase constitutes the malignant period of the infection, with abrupt or insidious onset, with chills, fever and sweating, joint and bone pain, hyperoxia, followed by severe anemia due to hemolysis, jaundice, hepatomegaly, lymph adenomegaly [7]. This phase may be less intense and, in some places, especially in Ecuador, it manifests very discreetly or goes unnoticed. It lasts between 2 to 4 weeks and the great majority of those who receive treatment recover. After an average of two months in this phase (which may not occur, particularly in natives of the endemic region) the Peruvian wart appears. The disease may not affect the skin in up to 45% of cases [8,9].
The chronic phase, eruptive or Peruvian wart, mainly affects children and adolescents, without a typical clinical picture of the acute hematic phase. Three types of lesions have been described: Miliary or papillary, represented by reddish papules, measuring lessthan 3 mm usually on the extremities. Subcutaneous nodules, with erythematous or normal overlying skin, scarce, located on the extensor surface of the extremities. The macular lesions are sometimes solitary neoformations, measuring 5 mm to 1-2 cm, erythematous, friable, sometimes pedunculated [9].
At the base of any of these lesions there is an epidermal collarette. The most common type of rash is milia, although different types may appear in the same patient. Miliary lesions are usually painless, whereas, the macular lesions may be painful and two thirds of the cases may bleed. Pruritus is variable. Spontaneously regressing lesions may also be observed, especially in children. Lesions in oral, conjunctival and nasal mucosa have been described. About 50% of patients with Peruvian warts are bacteremia. Without treatment, this phase persists from one month to one year, but the risk of becoming an asymptomatic reservoir is high, so in no case should the corresponding treatment be discontinued [9,10].
For diagnosis, in the febrile phase, the most useful technique is to obtain a blood smear (Giemsa-Wright staining). This method requires expertise. Sensitivity of 36% and specificity between 91 to 96% have been described; in the eruptive phase, the sensitivity of the smear is less than 10% [11].
Skin biopsy of the lesion remains the best method to confirm clinical suspicion in Peruvian wart. Histological alterations correspond to a hemangioid granulomatous reaction (telangiectatic granuloma). Other tests used are: PCR in blood and tissue samples and indirect immunofluorescence for the detection of antibodies [12].
Treatment depends on the stage of the disease: in cases of acute uncomplicated Bartonellosis, amoxicillin with clavulanic acid is recommended as first line therapy in pregnant women, children and adolescents under 14 years of age leaathan 45 kg, at a dose of 40 mg/kg/day p.o every 12 hours for 14 days, and ciprofloxacin for adults and older, heavier children, at a dose of 500 mg p.o every 12 hours for 14 days; as second line therapy, chloramphenicol, cotrimoxazole and amoxicillin [13]. Regarding complicated acute Bartonellosis, as first line therapy, IV ciprofloxacin and ceftriaxone and in pregnant women ceftriaxone with chloramphenicol and as second line, combinations of ciprofloxacin and ceftriaxone with ceftazidime and amikacin [14]. Likewise, in chronic eruptive Bartonellosis (Peruvian wart), the first line treatment in all cases is Azithromycin, in children and adolescents lessthan 45kg 10 mg/kg/day p.o x 7 days, in > 45 kg and adults 500 mg/day p.o x 7 days and in pregnant women, 1 g/day once a week x 3 weeks. As a second line of treatment: rifampicin, erythromycin and ciprofloxacin, the latter not indicated in pregnant women [13,14].
On the other hand, it is important to perform a clinical control of the lesions after 14 days to evaluate the therapeutic response, if this is good (decrease in number, size and color > 90%) the treatment is concluded, if it is regular (decrease in number, size and color between 50 and 90%) the therapy is extended with 1g of Azithromycin in a single dose. If there is no response (decrease in number, size and color lessthan 50%, or no change or new lesions appear), discontinue treatment and rotate second-line antibiotic [15]. In this study, we seek to report on a documented clinical case that allows us to identify the presence of Bartonella bacilliformis in a community of Ecuador.
A male patient, 13 years, 3 months old. Origin: rural area, San Pedro del Villao Enclosure. Pedro Carbo District. Guayas Province. Pathologic history: congenital heart disease, seen at the outpatient Dermatology clinic due to a clinical presentation suggestive of dermatosis, characterized by papules and nodules that sometimes bleed, of one year of evolution. On physical examination she presented with failure to thrive, afebrile, and several reddish papules and dry crusts, scattered in the right retro auricular region and limbs. In addition, an angiomatous tumor with desquamative collaret, located at the level of the third metacarpophalangeal joint; in the right gluteal fold, neoformation, friable, sessile, covered with blackish crust.

Figure 1: (A). Reddish tumor with desquamative collarette. (B). Neoformation with necrotic crust in gluteal fold and miliary lesion. (C). Erythematous papules on fingers. (D). Spontaneously regressing lesion.
Presumptive diagnoses: Peruvian wart vs. bacillary angiomatosis.
Tests performed: Normal blood biometry and peripheral blood smear. Normal liver and coagulation tests. Negative blood cultures. Blood sample: Negative Bartonella spp; PCR Gen rib C in skin sample (skin biopsy): Positive B. bacilliformis.
Treatment started: Azithromycin 500 mg p.o x 7 days. On day 14, she received 1g of the same drug as extended therapy, due to an 80 percentage decrease in lesions, achieving remission of the lesions with hypertrophic scarring at the biopsy site [10].

Figure 2: (A). Post-treatment lesion regression. (B). Post-treatment lesion regression.
2.1. Entomo-Epidemiological Activities
At the same time, the Epidemiological Surveillance team of the Hospital del Niño "Dr. Francisco de Icaza Bustamante" coordinated field actions with the Zonal and District teams of Health Coordinating Offices 8 and 5, respectively.
The entomological investigation consisted of placing CDC traps and capturing the vector in strategic locations in the house and surrounding areas. For this, we had the help of vector control personnel from Pedro Carbo Enclosure, who refer that this activity requires more time to complete the study, which would allow us to perform hourly activity and vector density.
It should be noted that, during field activities, by taking samples from relatives and neighbors, they reported that the patient frequented the area surrounding the house, which is adjacent to the mountain, a place where entomological research could be carried out in greater depth.

Figure 3: (A). Access to the San Pedro de Villao site. (B). Patient's home. (C). Stream.
The work team evaluated the ecosystem of the place and its surroundings. Pedro Carbo, is an enclosure located on the coast of Ecuador, near the province of Manabi. It is located at Km 63 of the Guayaquil-Manabí highway. The study area is located between 1°49'10" S and longitude 80°19'41 "W. The temperature at which the traps were placed fluctuated between 22 - 24o C and the relative humidity from 70 to 75%. The altitude of the site is 585 mts.
A great variety of exuberant vegetation, and houses surrounded by fruit trees (mango, tangerine, oranges and cotton) was observed. It shows the presence of permanent and semi-permanent bodies of water, such as streams, as well as animal tracks.
To evaluate vector density, traps were placed in the home and in two houses adjacent to the patient's home. In the remaining houses, three traps were placed per house (intradomicile, extra domicile and peridomicile). The traps were placed at 18:00HRS, for two consecutive days and removed HRS of the following day. Subsequently, they were sent to the National Vector Reference Center (CRNV) located at the Public Health Research Institute (INSPI- Quito) for classification and taxonomic identification of the species collected.
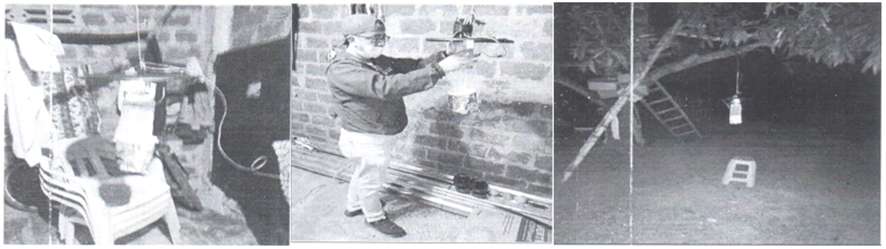
Figure 4: (A). Intra-domicile trap. (B). Peridomicile trap. (C). Extradomicile trap.

Figure 5: (A). Review of traps. (B). Surrounding house. (C). Surrounding river.
Eleven specimens belonging to the genus Lutzomia, and four species (cayennensis, gomenzi, sallesi and dysponeta) were taxonomically identified: none associated as a potential vector of B. bacilliformes.
B. bacilliformis is an opportunistic pathogen that is rarely isolated in clinical specimens and even more rarely in human blood [1]. It is the etiologic agent of Carrion's disease or Oroya fever (acute phase of infection) and Peruvian wart (chronic phase of infection) [1,3,4]. The acute phase of the disease is severe, characterized by a massive invasion of the bacteria into the erythrocytes and consequently causes acute hemolysis associated with fever [7]. If the infection is not treated, the mortality rate can reach up to 85% [10]. However, infection caused by this bacterium is rarely reported [8,9]. The chronic phase is characterized by benign pruritic and bleeding rash lesions and other symptoms such as malaise and osteoarticular pain [9]. At the time of admission to the local hospital, the patient was afebrile, with several reddish papules and dry crusts scattered in the right retro auricular region and extremities as obvious symptoms. In addition, an angiomatous tumor located at the level of the third metacarpophalangeal joint; in the right gluteal fold, neoformation, friable, sessile, covered with blackish crust.
B. bacilliformis can be isolated from blood cultures and secretions from lesions in people from endemic areas. B. bacilliformis infections are a health problem in many rural areas of South America (Andean Cordillera) and for travelers visiting these regions. Outbreaks of bartonellosis have been reported in the mountainous regions of Peru, Ecuador, and Colombia [3,4]. Since entomological surveillance of species of the Lutzomia genus is not carried out regularly as a surveillance system in the country, it is likely that for various reasons such as occupation, as well as man-vector contact due to the proximity of homes to the resting places of the vector, cases and colonization of the bacterium will continue to occur [5]. Human Bartonellosis or Carrion's disease continues to be a public health problem that, despite prevention and control efforts, persists in Ecuador, especially in rural and low-income areas similar to the patient's origin.
The patient's lesions decreased and returned to normal after treatment with Azithromycin. It is important to recognize the timeliness and timely diagnosis, which allowed for treatment efficacy and early recovery of the patient. [6]. It should be noted that the identification of the species using the PCR technique Gen ribC facilitated the correct administration of the treatment. Likewise, the patient under study was caught in the chronic (eruptive) phase of the disease, which is consistent with what the literature indicates, that this phase mainly affects children and adolescents [12]. Likewise, the evolution was favorable once the treatment was established and completed, taking into consideration the underlying pathology. At present, the patient continues with subsequent controls with the specialty.
From the above, it must be considered that B. bacilliformis multiplies rapidly in human reservoirs during the acute phase of the disease and remains for prolonged periods in convalescent persons [9,10]. The existence of wild reservoirs has not been demonstrated, being the sick and untreated man the only known reservoir. It should be noted that minors tend to have benign lesions, few in number and with a popular or miliary appearance, which can even involute spontaneously (becoming healthy carriers) [13].
In this regard, the current incidence of Bartonellosis shows seasonal and geographic variations, with an increase in cases during the rainy season. In addition, the lack of knowledge of the population and the difficulty in early diagnosis contribute to the spread of the disease. Addressing and reaching the correct diagnosis of Bartonellosis requires a comprehensive approach that includes the training of health professionals, access to laboratory tests, solid entomological and epidemiological surveillance, and continuous research to understand the reality of the country and consequent public education [14].
It is essential that governments and health institutions continue to invest in education, entomo-epidemiological surveillance and medical care programs to effectively address this disease that affects vulnerable communities.
There is currently a great silence about Carrion's disease, probably due to the low prevalence of cases at the national level in recent years.
In view of the above, it is imperative to raise awareness among the inhabitants of the localities where Lutzomia cohabits with human beings of the importance of knowing about this disease, which has special characteristics, especially in the infant population.
Ethical Approval
Ethical approval of the case report is not required as per local guidelines.
Consent
The patient was informed to the full extent of the use of their information and provided affirmative written consent for the publication of this case report and accompanying images.
Authors' Contributions
Glenda Velasquez, Boris Caballero, Gladys Colombia and Leyther Llanga, were involved in drafting of the manuscript. Adriana Sarango, was responsible for checking and reviewing the test data. Glenda Velasquez was responsible for the quality of the test data and the intercepted images. All authors approved the final draft for publication. Diana Berzina and Adriana Sarango, equally contributed to this work.
Recommendations
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.
