
Case Report | DOI: https://doi.org/10.31579/2690-8816/043
1 Department of Radiology, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria.
2 Department of Radiology, Federal Medical Center, Gusau, Nigeria.
*Corresponding Author: Muhammad SB, Department of Radiology, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria.
Citation: Ibrahim HG, Muhammad SB, Abubakar M, Hafsat AR and Joshua GK. (2021). A Giant Vesical Calculus in a Woman with Utero-Vaginal Prolapse: A Rare Case Report. J. Clinical Research Notes. 2(2). DOI: 10.31579/2690-8816/043
Copyright: © 2021 Muhammad SB. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 October 2021 | Accepted: 05 November 2021 | Published: 15 November 2021
Keywords: giant; calculus; woman; prolapse
Urinary bladder stone is usually defined as a giant calculus when it weighs 100g. The incidence of female urolithiasis is very low. According to literature, fewer than 2% of all bladder calculi occur in female subjects and thus, their presence should provoke careful assessment of the etiology.
H. A. is a 70 year old P10+2 2 alive woman from a rural community who presented to the Obstetrics and Gynecology Department of Usmanu Danfodiyo University Teaching Hospital Sokoto with 10 years history of protruding mass through the vagina and pain in passing urine of 1 year duration. No history of haematuria, fever or passage of stones in urine. Vaginal examination show an irreducible third degree uterine decent. Laboratory investigations revealed pus cells in urine and urine culture yielded growth of Escherichia Coli after overnight incubation. The electrolyte, urea and creatinine levels were normal.
On ultrasound, a large curvilinear echogenic structure that cast posterior acoustic shadowing consistent with calculus was demonstrated within the urinary bladder. It measured 4.5x3.7cm in size and showed marginal irregularities. The surrounding urine in the bladder show mobile internal echoes. Intravenous urogram showed a dense oval radio opaque calculus in the pelvis measuring about 4.5cm in diameter with normal upper urinary tract. She had open cystolithotomy with total abdominal hysterectomy. The stone weighs 142g.
Urinary bladder stone is usually defined as a giant calculus when it weighs 100g1. Urinary bladder calculi constitute 5% of all urolithiasis [2]. The incidence of female urolithiasis is very low. According to literature, fewer than 2% of all bladder calculi occur in female subjects and thus, their presence should provoke careful assessment of the etiology [3]. The association of vesical calculi and utero-vaginal prolapsed is an uncommon entity [4.5].
Radiography and ultrasound play a vital role in diagnosing this condition as well as evaluation of complications associated with it. We report a rare case of utero-vaginal prolapsed with large vesical calculus diagnosed by ultrasonography, plain radiography and intravenous urography.
H. A. is a 70 year old P10+2 2 alive woman from a rural community who presented to the Obstetrics and Gynecology Department of Usmanu Danfodiyo University Teaching Hospital Sokoto with 10 years history of protruding mass through the vagina and pain in passing urine of 1 year duration. No history of haematuria, fever or passage of stones in urine. She has been receiving drugs from a medicine vendor in her village but was never subjected to any type of investigation. No history of surgery in the past. She is a widow with two live female children. All her deliveries were at home and uneventful. No family history of utero-vaginal prolapse or bladder stone.
Physical examination show an elderly woman, malnourished. The abdomen was flat, soft, and non-tender. Vaginal examination show an irreducible third degree uterine decent. Laboratory investigations showed pus cells in urine and urine culture yielded growth of Escherichia Coli after overnight incubation. The electrolyte, urea and creatinine levels are within normal limits. The pack
cell volume was 30%. She was referred to radiology department to do abdomino-pelvic ultrasound and intravenous urography as part of pre-operative assessment.
On ultrasound, a large curvilinear echogenic structure that cast posterior acoustic shadowing consistent with calculus was demonstrated within the urinary bladder. It measured 4.5x3.7cm in size and showed marginal irregularities (figure1).
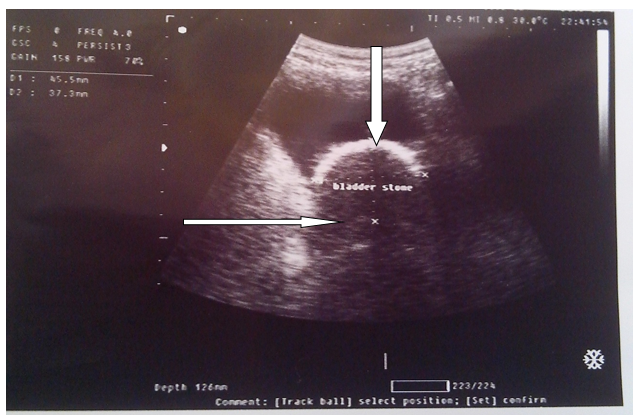
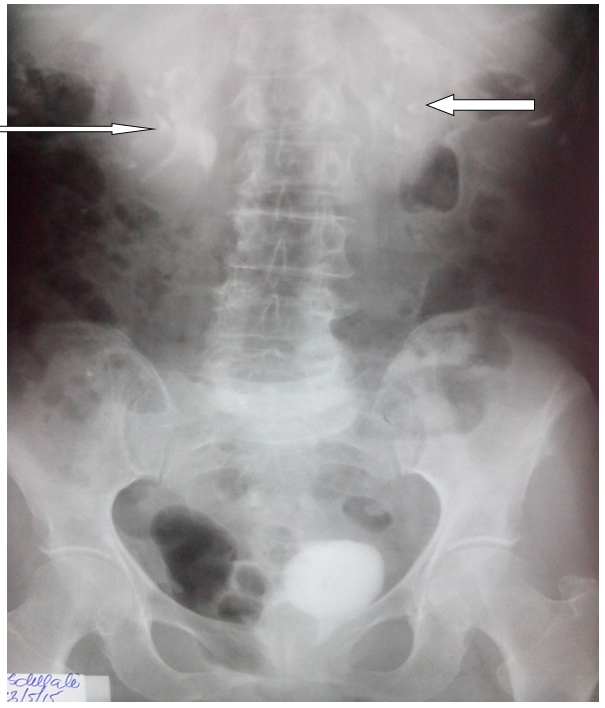
The surrounding urine in the bladder show mobile internal echoes. There was a simple renal cyst on the right side but no hydronephrosis or hydroureters was demonstrated. Plain radiograph showed a dense oval radio opaque calculus in the pelvis measuring about 4.5cm in diameter (figure 2).

On intravenous urogram, there was normal excretion of contrast medium by the kidneys on both sides with no features of hydronephrosis (figure 3).
The ureters were demonstrated in their entire length and are normal in positions and caliber. Urinary bladder view shows inferior displacement of the urinary bladder (figure 4).

Urinary bladder calculi are rare in women. Fewer than 2% of urinary bladder stone occur in females [3]. It is more often seen in the developing nations than the developed. Mungadi et al evaluate the pattern of urolithiasis in Sokoto North Western Nigeria in 121 patients. They reported that in 62% of cases the stones were solitary and they are seen more in males with a male to female ratio of 23.1:1 [6]. There have been a number of reports on bladder calculi in women with a history of gynecologic procedure [3, 7]. Long standing utero-vaginal prolapse and bladder outlet obstruction coupled with chronic infection are suspected to be the causative factors as demonstrated in this patient. Aside from the aforementioned causative factors, the predisposing factors that may cause the bladder stone in the present case were unique. The patient came from a very remote village that lacked a basic medical diagnostic facility which can be used to make the diagnosis early. The patient also had dietary problems along with reduced fluid intake. These factors probably compounded the urinary tract infection and resulted in the formation of the calculus. This findings tally with that of Rahman et al in Ilorin North West Nigeria [1].
Anatomical findings usually associated with vesical calculus in women are cystocele, enterocele of utero-vaginal prolapsed or findings of prior urethral surgery all of which contribute to elevated residual urine [4,5]. Bladder stone is one of the cause for irreducible utero-vaginal prolapsed sometimes as may be so in the index patient. As the uterus descends, the downward traction causes the bladder trigone and lower ureters to be dragged outside the pelvis. The caudal displacement of the trigone results in compression of the ureters between the uterus and medial borders of the genital hiatus. Complete uterine prolapsed results in an ‘hour glass’ configuration to the bladder as demonstrated in this case (figure 4).
The diagnosis of vesical calculi requires a high index of suspicion. A history of recurrent urinary tract infection with suprapubic pain that is aggravated by exercise, an interruption of the urinary stream and terminal haematuria are helpful but not pathognomonic of the disease because they may be caused by other lesions in the bladder.
Abdominal radiograph, ultrasonography, Intravenous urography (IVU) and computed tomography (CT) are the most useful tools in evaluation of vesical calculi [8]. Many clinicians use plain abdominal radiograph and ultrasound for initial studies. Ultrasound reveals many types of stones including some radiolucent stones and may yield other clinically important findings such as urinary obstruction, nephrocalcinosis or renal parenchymal disease. Danfulani et al demonstrated a giant bladder calculus in a child which shows features of early renal parenchymal disease on ultrasound. Our patient shows an associated simple right renal cyst on ultrasound. Bladder stones are usually single, large, rounded and of homogenous calcific density and thus evident on plain radiograph or on excretion urography with a contrast agent as demonstrated in our patient. Intravenous urography is however associated with higher radiation exposure and risk due to use of contrast agents. More recently studies have suggested that non enhanced helical CT is superior to IVU for the evaluation of urolithiasis. The advantage of CT includes shorter examination times, higher sensitivity and specificity for calculi, no need for intravenous contrast a greater potential for making alternative diagnosis [8].
Radiological findings associated with bladder calculus and utero-vaginal prolapse include internal echoes in the urine surrounding the calculus as observed in our case. Others include back pressure effect on the ureters and kidneys leading to hydroureters and hydronephrosis.
Open surgery with total abdominal hysterectomy has been the best recommended modality for large stones associated with utero-vaginal prolapse [4,5,8]. Other methods of bladder stone removal include extracorporeal shock wave lithotripsy and endoscopic cystolithotomy (transurethral or percutaneous). The success rate of extracorporeal shock wave lithotripsy ranges from 72-100% and it is a suitable method for patients with severe cormobidities [8,9]. In our patient the stone was large and she had open cystolithotomy with total abdominal hysterectomy.
Utero-vaginal prolapse is a common gynecological disorder in this environment. A long standing prolapse if untreated may lead to urinary tract complications such as bladder calculus. We reported a rare case of large bladder stone caused by long standing utero-vaginal prolapse evaluated by ultrasound, plain radiography and intravenous urography for which the patient had open cystolithotomy and hysterectomy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
