AUCTORES
Globalize your Research
Chat with us
Case Report | DOI: https://doi.org/10.31579/2690-4861/509
1Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, United States.
2St. George’s University School of Medicine, Grenada, Caribbean.
3Department of Radiation Oncology, American University of Beirut Medical Center, Beirut, Lebanon.
4University of Balamand, Balamand, Lebanon.
*Corresponding Author: Neal Kim, Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, United States.
Citation: Neal Kim, Zachary McSween, Lara Hilal, Joseph Hajj, Marsha Reyngold, et al., (2024), Reirradiation for De novo Anorectal Cancers in Patients with a History of Prostate Radiation Therapy: Dosimetric Considerations and Practical Radiation Planning Techniques, International Journal of Clinical Case Reports and Reviews, 18(5); DOI:10.31579/2690-4861/509
Copyright: © 2024, Neal Kim. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 July 2024 | Accepted: 01 August 2024 | Published: 09 August 2024
Keywords: prostate radiation therapy; anal cancer; rectal cancer; reirradiation; second course of pelvic RT; toxicity
This case report examines the treatment planning approach for patients receiving anorectal radiotherapy with a history of prostate radiotherapy. Three cases are presented: two of these patients received prior 50.4 Gy in 28 fractions via external beam radiation therapy, where one proceeded to obtain a cone-down of 30.6 Gy in 17 fractions, while the other received 100 Gy of low-dose-rate brachytherapy; the third patient only received prior low-dose-rate brachytherapy to an unknown dose due to absent prior planning records. This paper explores the unique challenges this reirradiation setting poses, outlines treatment planning strategies to overcome these obstacles, and reviews retreatment dose constraints from the literature.
RT, radiation therapy; EBRT, external beam radiation therapy; OAR, organ-at-risk; LDR, lose-dose rate; PTR, prior treatment review; IDL, isodose line; EQD2, equivalent dose in 2 Gy fractions; IMRT, Intensity-modulated radiation therapy; 3D-CRT, 3-dimensional conformal radiation therapy; GTV, gross tumor volume; PTV, planning target volume.
There is an increasing incidence of patients presenting with rectal cancer with a history of prostate radiotherapy [1]. There is no consensus about whether there is a direct relation between prior prostate radiotherapy and second pelvic cancer incidence. Omer et al. described common limitations in methodology among published studies, such as inconsistencies in defining the latency period and the extent of patient follow-up [2]. As prostate radiotherapy continues to advance and experience associated gains in survival paired with screening initiatives leading to earlier cancer diagnoses in younger patients, the option of pelvic reirradiation overall is expected to become an increasingly more common topic of consideration [2]. These cases can be particularly challenging for treatment planning as organs-at-risk (OARs) in pelvic reirradiation are primarily arranged in serial functional subunits, where injury to any segment of a serial organ can result in serious complications including, but not limited to, fistula formation, perforation, and radionecrosis [3,4].
This case report outlines the treatment planning approaches undertaken in managing this unique population at our institution. We selected three patients who recently received anorectal radiotherapy at our institution having a history of prostate radiotherapy. Two of the three patients received prior 50.4 Gy in 28 fractions via external beam radiation therapy (EBRT), where one received a cone-down of 30.6 Gy in 17 fractions of EBRT, and the other received 100 Gy of low-dose-rate (LDR) brachytherapy. The third patient received only prior LDR brachytherapy (dose unknown due to absent planning records). The patients’ differences in prior prostate radiotherapy modality led to their inclusion in this case study report as it resulted in diverging treatment planning considerations (see Table 1-3 for treatment summarization). We also compile pelvic reirradiation constraints cited in the literature with their corresponding interval between radiation courses, follow-up interval, and Grade 3+ toxicity incidences to contextualize our cases better and provide insight on best practices to manage this unique patient population (see Tables 4-6).
| Case | Prostate RT | Pelvic RT | Initial Clinical Response | In-field POD | Out-of-field POD | Grade 3+ Toxicity | OS from RT end |
| 1 | 2012: -EBRT 50.4 Gy/28 fx + 30.6 Gy/17 fx | 2022: -Anorectal + LN 50/45 Gy/25 fx QD | Partial | No POD | 8 mo; skin (Merkel cell) | Grade 3 acute dermatitis | 11 mo |
| 2 | 2001: -EBRT 50.4 Gy/28 fx + 100 Gy LDR | 2022: -Rectum + LN 45 Gy/30 fx BID | Complete | No POD | No POD | N | 17 mo (since last f/u) |
| 3 | 2001: -LDR dose unavailable | 2017: -Rectum + LN 45 Gy/25 fx QD | Complete | No POD | No POD | N | 60 mo |
Table 1. Treatment characteristics
Table 1 Abbreviations: RT, radiation therapy; POD, progression of disease; OS, overall survival; EBRT, external beam radiation therapy; LN, lymph nodes; QD, once a day; LDR, low-dose-rate (brachytherapy); BID, = twice a day; f/u, follow-up.
| Case | Structure | Prior-RT Brachytherapy Dmax Gy3 EQD2 | Prior-RT EBRT Dmax Gy3 EQD2 | Re-RT Dmax Gy3 EQD2 | Total Gy3 EQD2 |
| 1 | Bladder | 77.8 | 46.2 | 123.9 | |
| Rectum | 77.8 | 55.2 | 133 | ||
| Urethra | 77.8 | 31.8 | 109.6 | ||
| 2 | Bladder | 47.8 (D2cc) | 60.7 | 40.5 | 149 |
| Rectum | 47.8 (D2cc) | 55.7 | 40.5 | 143.9 | |
| Urethra | 47.8 (D2cc) | 55.2 | 40.5 | 143.5 | |
| 3 | Bladder | N/A | 50.5 | N/A | |
| Rectum | N/A | 50.7 | N/A | ||
| Urethra | N/A | 13.3 | N/A |
Table 2. Dosimetric details
Table 2 Abbreviations: RT, radiation therapy; EQD2, equivalent dose in 2 Gy fractions.
| Case | Planning Scan | Fusion | Contrast | Orientation | Immobilization | Anal BB Marker | Foley Catheter | Full Bladder | Imaging |
| 1 | CT | PET | IV & Oral | Head-first supine (Frog-leg) | Alpha cradle | Y | N | Y | Every treatment, 2D kV Imaging |
| 2 | MRI T1 & T2 | IV | Head-first prone | Belly board | Y | ||||
| 3 | N | N | Head-first prone | Belly board | N |
Table 3. Simulation and setup details
| Structure | n | Metric | Median Gy3 EQD2 | Range | Interquartile Range |
| Bladder & Bladder wall | 10 | Dmax-D1cc < | 116.3 | 80-147.4 | 110-137.1 |
| Rectum & Rectal wall | 14 | Dmax-D1cc < | 124.5 | 88.4-169.2 | 111.5-137.4 |
| Urethra | 9 | Dmax-D1cc < | 144.8 | 134.1-165.1 | 144.8-158.8 |
Table 4. Summary of cumulative dose constraints
Table 4 Abbreviations: EQD2, equivalent dose in 2 Gy fractions.
| OAR | Re-RT Cited Constraint | Re-RT Rx (Median) | Re-RT Constraint in EQD2 | (Estimated) Prior-RT Rx (Median) | Cumulative Constraint in EQD2 |
| Bladder11 | Dmax < 36 Gy | 30 Gy/5 fx | Dmax < 73.4 Gy3 EQD2 | N/A | Dmax < 147.4 Gy3 EQD2 |
| Bladder wall12 | Dmax < 34 Gy | 34 Gy/5 fx | Dmax < 66.6 Gy3 EQD2 | 75.6 Gy/40 fx | Dmax < 140.6 Gy3 EQD2 |
| Bladder wall13 | Dmax < 34 Gy | 34 Gy/5 fx | Dmax < 66.6 Gy3 EQD2 | 73.8 Gy/40 fx | Dmax < 138.1 Gy3 EQD2 |
| Bladder10 | Dmax < 110 Gy3 EQD2 | Dmax < 110 Gy3 EQD2 | |||
| Bladder14 | Dmax < 25 Gy | 25 Gy/5 fx | Dmax < 40 Gy3 EQD2 | 50.4 Gy/28 fx | Dmax < 88.4 Gy3 EQD2 |
| Bladder15 | D0.1cc < 33 Gy | 36-38 Gy/6 fx | D0.1cc < 56.1 Gy3 EQD2 | 78 Gy/39 fx | D0.1cc < 134.1 Gy3 EQD2 |
| Bladder16 | D0.5cc < 80 Gy3 EQD2 | D0.5cc < 80 Gy3 EQD2 | |||
| Bladder15 | D0.5cc < 28 Gy | 36-38 Gy/6 fx | D0.5cc < 42.9 Gy3 EQD2 | 78 Gy/39 fx | D0.5cc < 120.9 Gy3 EQD2 |
| Bladder16 | D0.5cc < 110 Gy3 EQD2 | D0.5cc < 110 Gy3 EQD2 | |||
| Bladder15 | D1cc < 24 Gy | 36-38 Gy/6 fx | D1cc < 33.6 Gy3 EQD2 | 78 Gy/39 fx | D1cc < 111.6 Gy3 EQD2 |
| Rectum17 | Dmax < 40 Gy | 30 Gy/5 fx | Dmax < 88 Gy3 EQD2 | 70 Gy/25 fx | Dmax < 169.2 Gy3 EQD2 |
| Rectum18 | Dmax < 40.5 Gy | 36 Gy/6 fx | Dmax < 79 Gy3 EQD2 | 74 Gy/40 fx | Dmax < 150.8 Gy3 EQD2 |
| Rectal wall12 | Dmax < 34 Gy | 34 Gy/5 fx | Dmax < 66.6 Gy3 EQD2 | 75.6 Gy/40 fx | Dmax < 140.6 Gy3 EQD2 |
| Rectal wall13 | Dmax < 34 Gy | 34 Gy/5 fx | Dmax < 66.6 Gy3 EQD2 | 73.8 Gy/40 fx | Dmax < 138.1 Gy3 EQD2 |
| Rectal wall17 | Dmax < 30 Gy | 30 Gy/5 fx | Dmax < 54 Gy3 EQD2 | 70 Gy/25 fx | Dmax < 135.2 Gy3 EQD2 |
| Rectum11 | Dmax < 30 Gy | 30 Gy/5 fx | Dmax < 54 Gy3 EQD2 | N/A | Dmax < 128 Gy3 EQD2 |
| Rectum19 | Dmax < 22.5 Gy | 30 Gy/5 fx | Dmax < 33.8 Gy3 EQD2 | 80 Gy/40 fx | Dmax < 113.8 Gy3 EQD2 |
| Rectum10 | Dmax < 100 Gy3 EQD2 | Dmax < 100 Gy3 EQD2 | |||
| Rectum20 | Dmax < 22.5 Gy | 30 Gy/5 fx | Dmax < 33.8 Gy3 EQD2 | 66 Gy/33 fx | Dmax < 99.8 Gy3 EQD2 |
| Rectum14 | Dmax < 25 Gy | 25 Gy/5 fx | Dmax < 40 Gy3 EQD2 | 50.4 Gy/28 fx | Dmax < 88.4 Gy3 EQD2 |
| Rectum15 | D0.1cc < 33 Gy | 36-38 Gy/6 fx | D0.1cc < 56.1 Gy3 EQD2 | 78 Gy/39 fx | D0.1cc < 134.1 Gy3 EQD2 |
| Rectum15 | D0.5cc < 28 Gy | 36-38 Gy/6 fx | D0.5cc < 42.9 Gy3 EQD2 | 78 Gy/39 fx | D0.5cc < 120.9 Gy3 EQD2 |
| Rectum21 | V36 < 1cc | 35-36.25 Gy/5 fx | V73.4 Gy3 EQD2 < 1cc | 70 Gy/40 fx | V141.3 Gy3 EQD2 < 1cc |
| Rectum15 | D1cc < 24 Gy | 36-38 Gy/6 fx | D1cc < 33.6 Gy3 EQD2 | 78 Gy/39 fx | D1cc < 111.6 Gy3 EQD2 |
| Urethra12 | Dmax < 40.8 Gy | 34 Gy/5 fx | Dmax < 91.1 Gy3 EQD2 | 75.6 Gy/40 fx | Dmax < 165.1 Gy3 EQD2 |
| Urethra13 | Dmax < 40.8 Gy | 34 Gy/5 fx | Dmax < 91.1 Gy3 EQD2 | 73.8 Gy/40 fx | Dmax < 162.6 Gy3 EQD2 |
| Urethra19 | Dmax < 37.5 Gy | 30 Gy/5 fx | Dmax < 78.8 Gy3 EQD2 | 80 Gy/40 fx | Dmax < 158.8 Gy3 EQD2 |
| Urethra17 | Dmax < 36 Gy | 30 Gy/5 fx | Dmax < 73.4 Gy3 EQD2 | 70 Gy/25 fx | Dmax < 154.6 Gy3 EQD2 |
| Urethra11 | Dmax < 36 Gy | 30 Gy/5 fx | Dmax < 73.4 Gy3 EQD2 | N/A | Dmax < 147.4 Gy3 EQD2 |
| Urethra20 | Dmax < 37.5 Gy | 30 Gy/5 fx | Dmax < 78.8 Gy3 EQD2 | 66 Gy/33 fx | Dmax < 144.8 Gy3 EQD2 |
| Urethra15 | Dmax < 33 Gy | 36-38 Gy/6 fx | Dmax < 56.1 Gy3 EQD2 | 78 Gy/39 fx | Dmax < 134.1 Gy3 EQD2 |
| Urethra22 | V36 < 1cc | 30 Gy/5 fx | V73.4 Gy3 EQD2 < 1cc | N/A | V147.4 Gy3 EQD2 < 1cc |
| Urethra23 | V36 < 1cc | 36 Gy/6 fx | V64.8 Gy3 EQD2 < 1cc | 75.6 Gy/40 fx | V138.7 Gy3 EQD2 < 1cc |
Table 5. Individual cumulative dose constraints
Table 5 Abbreviations: RT, radiation therapy; Rx, prescription; EQD2, equivalent dose in 2 Gy fractions.
| Source | Median Prior and Re-RT Interval | Median Re-RT Follow-up Interval | Grade 3+ Toxicity | Comments |
| Abusaris (2011)10 | Between 1st & 2nd course, 15 mo (1.5-81.5); between 2nd & 3rd course, 7 mo (1.5-40) | After 2nd course, 16 mo (7.5-57); after 3rd course, 7 mo (3.5-49.5) | (n=23) After three radiation courses, 4% of the patients experienced acute Grade 3 pain and 7% of the patients acute Grade 3 dysuria. Grade 3 late skin toxicity was experienced in 4% of the patients. | Cumulative constraint directly cited in Gy3 EQD2. Note that these values are adjusted for time (i.e., dose reduction of 25/50% for a re-irradiation after 6-12 months/12 months+, respectively). |
| Loi (2018)11 | 76 mo (9-205) | 21.3 mo (6.1-49.2) | (n=50) One patient experienced both Grade 3 acute and chronic bladder toxicity, consisting of acute urinary retention and macro-hematuria, respectively. | Prior RT: Median Rx dose = 74 Gy4 EQD2 (60-80). Fractions unspecified, though likely close to 2 Gy/fx and calculating for using Gy3 EQD2 a/b = 3 should yield similar value. |
| Fuller (2020)12 | 98 mo (31-241) | 44 mo (3-110) | (n=50) Late toxicity was limited to the GU domain, with 5-year Grade 3+ GU rates of 8%. | Prior RT: Median Rx dose = 75.6 Gy (64.8-81). Fractions unspecified, though 92% received conventionally fractionated RT, thereby 40 fx estimated for calculation. |
| Fuller (2015)13 | 88 mo (32-200) | 24 mo (3-60) | (n=29) One patient with acute and late Grade 3 toxicity (urethral obstruction with suprapubic catheter, hemorrhagic cystitis), and one with late Grade 4 toxicity (hemorrhagic cystitis with subsequent cystoprostatectomy). | Prior RT: Median Rx dose = 73.8 Gy (64.8-81). Fractions unspecified, though expect mostly conventionally fractionated based on paper context, thereby 40 fx estimated for calculation. |
| Dagoglu (2015)14 | 22 mo (15-336) | 38 mo (6-86) | (n=18) One patient had small bowel perforation and required surgery (Grade 4), two patients had symptomatic neuropathy (one Grade 3) and one patient developed hydronephrosis from ureteric fibrosis requiring a stent (Grade 3). | Prior RT: Median Rx dose = 50.4 Gy (25-100.4). Fractions unspecified, though expect mostly conventionally fractionated based on paper context, thereby 28 fx estimated for calculation. |
| Bergamin (2020)15 | 99.6 mo (54-163.2) | 25 mo (13-46) | (n=25) There was one Grade 3 GI toxicity (4%), who developed tenesmus 60 days post reirradiation and was found to have a rectal ulcer overlying the hydrogel. | Prior RT: Median Rx dose expected = 78 Gy. Fractions unspecified, though expect mostly conventionally fractionated based on paper context, thereby 40 fx estimated for calculation. |
| Slevin (2021)16 | Consensus paper. Cumulative constraint cited directly in Gy3 EQD2. Note that for the constraint Bladder D0.5cc < 80 80 Gy3 EQD2 as “ideally and assuming no recovery,” 72% of experts agreed-strongly agreed, which was considered “not consensus.” | |||
| Cozzi (2023)17 | 73.8 mo (21-146) | 26.7 mo (7-50) | (n=20) No ≥ Grade 3 GU/GI acute/late toxicities reported. | Prior RT: Median Rx = 70 Gy (35-78.2)/25 fx (5-39). |
| Scher (2019)18 | 82.5 mo (29-207) | 21 mo (3-31) | (n=42) One patient experienced Grade 3 acute and late urinary toxicity (urinary incontinence). | Prior RT: Median Rx dose = 74 Gy (65-76). Fractions unspecified, though 83% were treated with 3D-CRT, thereby 40 fx estimated for calculation. |
| Vavassori (2010)19 | From biochemical failure to re-RT: 13.5 mo (2.7-38.4) | 11.2 mo (9.6-18.6) | (n=6) No ≥ Grade 3 GU/GI acute/late toxicities reported. | Prior RT: Median Rx dose = 80 Gy (70-80). Fractions unspecified, though expect mostly conventionally fractionated based on paper context, thereby 40 fx estimated for calculation. |
| Arcangeli (2015)20 | 36 mo | 6 mo | (n=1) No ≥ Grade 3 GU/GI acute/late toxicities reported. | Prior RT: Rx = 66 Gy/33 fx, though n=1. |
| Janoray (2016)21 | 11.7 mo (2.5-46.5) | 111 mo (38-398) | (n=21) No ≥ Grade 3 GU/GI acute/late toxicities reported. | Prior RT: Median Rx dose = 71.1 Gy (45-76.5). Fractions unspecified, though expect mostly conventionally fractionated based on paper context, thereby 40 fx estimated for calculation. |
| Michalet (2022)22 | 88 mo (21-240) | 12 mo | (n=33) One patient experienced a Grade 3 hematuria requiring an intervention. | Prior RT: Median Rx dose = 74 Gy EQD2. Fractions and a/b unspecified, though physical Rx dose ranged from 66-80, and calculating for using Gy3 EQD2 a/b = 3 should yield similar value. |
| Leroy (2017)23 | 65 mo (28-150) | 22.6 mo (6-40) | (n=23) Two patients presented with Grade 3 toxicities (two cystitis and one neuralgia) | Prior RT: Median Rx dose = 75.6 Gy (70-75.6). Fractions unspecified, though expect mostly conventionally fractionated based on paper context, thereby 40 fx estimated for calculation. |
Table 6. Reirradiation outcomes
Table 6 Abbreviations: RT, radiation therapy; Rx, prescription; EQD2, equivalent dose in 2 Gy fractions; fx, fractions; GU, genitourinary; GI, gastrointestinal; 3D-CRT, 3-dimensional conformal radiation therapy.
Our institution follows a general workflow when addressing reirradiation cases for planning, referred to as prior treatment review (PTR). When target volumes are finalized by the radiation oncologist, a medical physicist or dosimetrist planner initiates PTR by first assessing the overlap between the prior and current treatments. This step can be limited due to the need for prior planning records that relevant treatment parameters and dosimetry, such as dose-volume histograms (DVHs), digitally reconstructed radiographs (DRRs), and isodose distributions. This limitation is often associated with prior radiotherapy delivered at an outside institution. In contrast, patients previously treated in-house have their plans readily accessible to assess treatment overlap more reliably by reproducing treatment fields, isodoses, and structures on the reirradiation CT simulation scan. The degree of treatment overlap is communicated to the radiation oncologist. It may result in changes to the target volume/field aperture, isodose distribution, and prescription dose/fractionation to meet retreatment constraints. These are defined in equivalent dose in 2 Gy fractions (EQD2) and utilized for reirradiation cases cross-campus-wide for a given anatomical site.
Planners can convert between physical dose and EQD2 using the following equation [5]:
Equation 1
Where D is the total physical dose (Gy), d is the physical dose per fraction (Gy), and α/β ratio refers to the responsivity of a given tissue to cell killing. The cumulative dose received by an OAR can be calculated by summing the doses, often for the maximum dose (Dmax), in Gy EQD2 from every prior plan and the proposed current plan, at which this cumulative value should be less than the retreatment constraint in question. If the constraint is exceeded, consensus must be achieved with another radiation oncologist with site expertise in a peer review process before the patient can start treatment.
An 80-year-old male with a past medical history of prostate cancer (cT1cN0M0) underwent a colonoscopy in 2022. A rectal mass was discovered, and a biopsy revealed a moderately to poorly differentiated adenocarcinoma with mucinous features. Perineal and digital rectal exams revealed a fungating lesion starting at the anal verge that extended to the anal margin and involved the sphincter. CT showed a 3.4x2.9cm perianal mass at the sphincter complex without metastases, staged as locally advanced anorectal adenocarcinoma. The patient was shortly started on neoadjuvant FOLFOXx8. The patient declined abdominoperineal resection to preserve the sphincter and instead opted for definitive radiation with concurrent 5-fluorouracil.
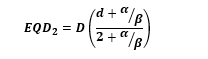
In the latter half of 2022, the patient underwent a CT/PET simulation: positioned supine in a frog-leg position, immobilized using an alpha cradle, with a full bladder, and without a Foley catheter. The patient was prescribed 45 Gy in 25 fractions to the pelvic lymph nodes (PTV45) and simultaneously boosted the anorectal region to 50 Gy (PTV50). PTV45 included the perirectal, presacral, internal iliac, external iliac, and inguinal nodes. PTV50 was generated from an expansion of the anal canal and the connecting partial segment of the rectum (see Figure 1A). EMR documentation revealed that the patient received prostate EBRT in 2012 at an outside institution, delivering a total of 81 Gy in 45 fractions via IMRT: 50.4 Gy in 28 fractions were delivered to the prostate and seminal vesicles, followed by a cone-down of 30.6 Gy in 17 fractions delivered to the prostate alone. This was the extent of prior treatment information, as planning records were unavailable.
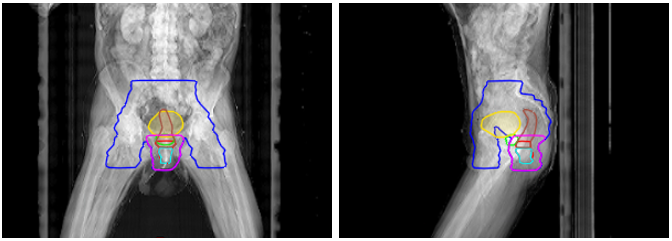
Figure 1A: Case report 1: yellow = bladder, brown = rectum, teal = anal canal, red = GTV, blue = PTV45, magenta = PTV50, and green = prostate.
The prior target was assessed to have largely overlapped with the current treatment, and for calculating cumulative dose, the prior contribution to OARs was assigned 81 Gy, i.e., to have received a Dmax of the prior prescription. Our intuition’s retreatment constraints for genitourinary (GU) are higher than that of gastrointestinal (GI), where for GU: bladder and rectum Dmax < 150 and 140 Gy3 EQD2, respectively; for GI: both bladder and rectum Dmax < 100 Gy3 EQD2. Reirradiation cases discussed in this study can be considered a blend of these two categories, and from a planning perspective, questions arise on which retreatment constraint values to use. Following peer review, delivering full prescription coverage was determined acceptable, where the bladder and rectum received a Dmax of 123.9 and 133 Gy3 EQD2, respectively. The urethra and prostate were also limited to Dmax < 110 and 120 Gy3 EQD2, respectively, in concern of urinary complications. This resulted in some
compromise of target coverage: V100% of GTV and PTV50 were 98.1% and 92.6%, respectively; D95% of GTV and PTV50 were 101.7% and 97.0%, respectively.
About two-thirds into the treatment course, the patient notably experienced diarrhea (4-6 stools per day over baseline) and moist desquamation not confined to the skin folds (Grade 3 acute dermatitis), which was treated with Silvadene and resolved mostly by the time of completion of radiotherapy. After fraction 22 of 25, the patient was admitted to a hospital for severe acute respiratory syndrome, and chemoradiation was paused for one month before proceeding to deliver the remaining fractions. Four months after completing radiotherapy, the patient reported feeling significantly better without any significant rectal or urinary issues. A sigmoidoscopy and CT around this time showed partial clinical response without evidence of new disease. The patient was shortly started on capecitabine but could not tolerate it due to severe diarrhea, which required an 11-day admission at a local hospital. At the eight-month mark, the patient was diagnosed with Merkel cell carcinoma via biopsy. This presented as subcutaneous nodules across the lower abdomen to the bilateral groins and pubis, and the patient was experiencing unbearable pain. The patient was started on carboplatin etoposide in response, but treatment was stopped indefinitely within two months due to his rapidly deteriorating condition. The patient passed away shortly afterward, which was approximately 11 months after the completion of pelvic reirradiation, and has experienced Grade 3+ toxicity in acute dermatitis.
An 87-year-old man with a past medical history of prostate cancer underwent a colonoscopy in 2022. An ulcerated, non-obstructive rectal mass was discovered, and biopsy results revealed moderately differentiated adenocarcinoma of the rectum. MRI showed a tumor that was 4.1cm in craniocaudal length, 7.4cm distance between the inferior border to the anal verge, staged as cT4bN+M0. The patient was started on neoadjuvant FOLFOXx8. As a poor surgical candidate, the patient opted to pursue definitive radiation with concurrent capecitabine.
Later that year, the patient underwent a CT simulation: positioned prone on a belly board, with a full bladder and no Foley catheter. A same-day MRI was obtained, to which the T1 and T2 sequences were fused to the planning CT scan. The patient was prescribed 45 Gy in 30 fractions BID [6] to both the rectum and pelvic lymph nodes (PTV45), which included the perirectal, presacral, internal iliac, and external iliac nodes (see Figure 1B). EMR documentation revealed that the patient received prostate-only EBRT followed by brachytherapy in 2005 at an outside institution. IMRT was used to deliver 50.4 Gy in 25 fractions, followed by 100 Gy LDR brachytherapy via Pd-103 seeds.
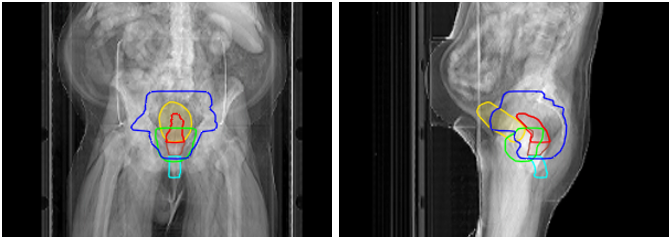
Figure 1B: Case report 2: yellow = bladder, brown = rectum, teal = anal canal, red = GTV, blue = PTV45, magenta = PTV50, and green = 50% IDL of brachytherapy.
Unlike prior EBRT doses seen with Case Report 1, Equation 1 cannot calculate EQD2 for LDR brachytherapy as there are no fractions, lacking the variable “d” (dose per fraction). Hilal et al. circumvent this, building upon the methodology outlined in Stock et al., using Equations 2and 3 below to first calculate BED and then convert to EQD2 [1,7]:

Equation 2
Where λ is the radioactive decay constant, calculated from ln(2)/T1/2, where T1/2 is the radioisotope’s half-life, and μ is the repair rate constant, calculated from ln(2)/t1/2, where t1/2 is the tissue repair half-time. Stock et al. specify T1/2 and t1/2 for Pd-103 as 17 days and 1 hour, respectively, used for brachytherapy calculations in this paper [7]. The BED is then converted to EQD2 through the following equation (rearrangement of Equation 1):

Equation 3
Utilizing the prior plan reports, Dmax to the bladder, rectum, and urethra were 148, 150, and 158 Gy3, which are 99.5, 101, and 107 Gy3 EQD2, respectively, after applying Equations 2 and 3. When summed with the prior combination EBRT doses, the bladder, rectum, and urethra total 160.2, 156.7, and 162.2 Gy3 EQD2, respectively. Therefore, the contribution of EQD2 from only the prior radiotherapy course exceeds the GU retreatment constraints used at our institution (bladder and rectum Dmax < 150 and 140 Gy3 EQD2, respectively) before even factoring in current doses. TG-137 recommends reporting brachytherapy doses that D2cc rather than Dmax act as the primary planning parameter when evaluating rectum dose [8]. Their rationale is that D2cc of irradiated volume is more clinically relevant over D0.1cc (a proxy for Dmax), which is instead listed as a secondary parameter [8]. Applying that understanding here, when D2cc is used for prior brachytherapy doses delivered (approx. 75 Gy), prior bladder, rectum, and urethra doses total 108.5, 103.4, and 103 Gy3 EQD2, respectively.
Between peer review and consensus with the brachytherapy team, the consensus was to reproduce the 50% (50 Gy) isodose line (IDL) of the brachytherapy treatment achieved in part by referencing the prior plan report’s dose distribution and considering the current anatomy and position of the prostate and seed implants. This region was limited to D1cc < 45 Gy and resulted in some compromise of target coverage: V100% of GTV and PTV45 were 60.2% and 83.2%, respectively; D95% of GTV and PTV45 were 90.9% and 90.6%, respectively; Dmin of GTV was 87.9% (39.6 Gy). Note that PTV45 comprises the rectum and pelvic lymph nodes, as the structure set did not contain a separate PTV for only the rectum. Optimizing the dose distribution in this manner also resulted in lesser doses to the urethra and prostate. As the prior 50% brachytherapy IDL was mainly limited to less than 45 Gy, the bladder, rectum, and urethra could be said to have received 40.5 Gy3 EQD2, which would total 149, 143.9, and 143.5 Gy3 EQD2, respectively.
By the end of the radiotherapy treatment course, the patient had notably experienced hemorrhoids, diarrhea (4-6 stools per day over baseline), and fatigue limiting instrumental ADL. One month after radiotherapy, the patient was admitted to a local hospital for four days, receiving treatment for colitis with IV Flagyl after initially presenting at their emergency department for fatigue, weakness, and persistent loose stools. At the six-month mark, the patient reported a significant improvement in overall well-being and denied any pain, diarrhea, or blood in the stool. Sigmoidoscopy and MRI findings at this time were consistent with a complete clinical response. The patient showed no evidence of disease or side effects during the latest follow-up visit, which was approximately 17 months after the completion of pelvic reirradiation and has not experienced radiotherapy-related Grade 3+ toxicity.
An 86-year-old male with a past medical history of prostate cancer (T1c) underwent a colonoscopy in 2017. A large 7.0cm mass was seen in the rectum extending to the dentate line, where biopsy revealed invasive moderately differentiated adenocarcinoma. MRI revealed a partially circumferential tumor 3.3cm in craniocaudal length and 3.0cm from the inferior border to the anal verge, staged as cT3N0M0. The patient was deemed to have high surgical risk due to needing to stop Plavix and opted for definitive radiation with concurrent capecitabine.
Later, in 2017, the patient underwent a CT simulation: positioned prone on a belly board without a full bladder and Foley catheter. The patient was prescribed 45 Gy in 25 fractions to both the rectum and pelvic lymph nodes (PTV45), which included the perirectal, presacral, internal iliac, external iliac, and inguinal nodes (see Figure 1C). EMR documentation revealed that the patient received prostate LDR brachytherapy in 2001 at an outside institution via Pd-103 seeds. However, no prior planning records were available, including mention of the prescription dose, which limited the calculation of prior EQD2.

Figure 1C: Case report 3: yellow = bladder, brown = rectum, teal = anal canal, red = GTV, blue = PTV45, magenta = PTV50, and
green = PRV prostate.
The radiation oncologist had contoured the prostate and applied an isotropic margin of approximately 0.6cm to create “PRV_prostate,” to which 25 Gy was minimized to this region and is similar in concept to the 50% IDL region seen with Case Report 2. PRV_prostate was kept to D1cc = 2344.8 cGy, resulting in some compromise of target coverage: V100% of GTV and PTV45 were 68.1% and 98.4%, respectively; D95% of GTV and PTV45 were 43.6% and 102.5%, respectively; Dmin of GTV was 33.3% (14.5 Gy). Note that PTV45 was cropped some margin from PRV_prostate such that some GTV extended outside PTV45. Also, note that PTV45 comprises both the rectum and pelvic lymph nodes, as the structure set did not contain a separate PTV for only the rectum. The bladder, rectum, and prostate (no urethra contoured) received a Dmax of 50.5, 50.7, and 13.3 Gy3 EQD2, respectively.
The patient tolerated treatment well overall, experiencing some fatigue and diarrhea during the last week of the radiotherapy. Around one-and-a-half months afterwards, the patient underwent sigmoidoscopy, revealing findings consistent with a complete clinical response and supported by an MRI suggesting radiological response. The patient did not have any major symptoms around this time, though the patient remained on active surveillance in consideration of his age and comorbid condition. At the three-month mark, the patient was started on four months of adjuvant capecitabine. The patient tolerated the first two cycles very well, but treatment was paused after the third cycle due to increasing toxicity impacting his quality of life, involving fatigue, diarrhea, and hand-foot syndrome. Treatment was stopped indefinitely when the patient incurred a pelvic fracture from a fall that required prolonged rehabilitation and went on active surveillance. In 2022, the patient was admitted to a local hospital and diagnosed with aspiration pneumonia and COVID-19. The patient passed away several days later, which was approximately 60 months after the completion of pelvic reirradiation. The patient showed ongoing complete clinical response during his last follow-up visit and did not experience radiotherapy-related Grade 3+ toxicity.
Minimizing OAR late toxicity is a top priority in a reirradiation setting. The process at our institution involves a PTR utilizing cumulative retreatment constraints, which aim to achieve consistent treatment planning outcomes for these complex cases. Considering that modern radiotherapy delivery techniques allow for PTV isodose “carving” such that OARs interfacing PTVs can be prioritized to receive significantly less than the prescription dose, creating a heterogeneous dose with a sharp gradient at the OAR interface. Retreatment constraints cited in the literature can better reflect the cumulative doses actually received by nearby OARs. We searched the literature for any direct mention of pelvic retreatment constraints, and many were compiled in Murray et al. and Baty et al. [4,9]. Constraints ranging from Dmax to D1cc (Dmax-D1cc) were selected, rewritten in terms of Gy3 EQD2, and added to their prior prescription dose in Gy3 EQD2 to approximate a cumulative dose constraint.
When referring to the information in Tables 4-6, we should recognize the interplay of variables that can help contextualize the results of this case report summarized in Tables 1-3. First, reirradiation prescriptions cited in the literature were predominantly hypofractionated, whereas the cases in this study were delivered in 25-30 fractions. Hyperfractionation in the context of pelvic reirradiation is seen increasingly utilized at our institution, delivering 39-45 Gy in 1.5 Gy/fx BID 6-8 hours apart, as it should offer greater interfractional normal tissue repair [6]. The interval between prior and reirradiation is another variable worth considering as it may indicate some degree of normal tissue recovery, where Abusaris et al. had allowed up to 50% of the prior EQD2 delivered to be subtracted when determining cumulative dose depending on this interval [10]. From a dosimetric perspective, the cumulative dose constraints seen in Table 4-5 were calculated assuming Dmax-D1cc as the prior prescription, whereas these were likely closer to 110% of the prescription considering that the prior radiotherapy technique was often 3D-CRT; this adds a buffer element to those cumulative values. Lastly, between prior prostate radiotherapy and anorectal reirradiation, the locations of Dmax-D1cc are more likely to overlap at distinct locations, unlike with prostate reirradiation, to which the constraints in Table 4-5 are largely tailored. When accounting for the variables described above, the approach and doses seen in our cases align more closely with that of the literature: the median Dmax-D1cc for bladder & bladder wall (n=10) < 116.3 Gy3 EQD2 (range: 80-147.4), rectum & rectal wall (n=14) < 124.4 Gy3 EQD2 (range: 88.4-160.2), and urethra (n=9) < 147.4 Gy3 EQD2 (range: 134.1-165.1), summarized in Table 4.
To improve PTR at our institution, we should expand our retreatment procedures and constraints to include this paradigm of patients, particularly for patients who have received prior combination brachytherapy and EBRT. Additionally, the limitation of unavailable prior planning records should lessen over time as patients’ first course of radiotherapy is delivered in modern times when EMR and TPS are standard for radiation oncology clinics. This will enable a more consistent and thorough PTR and improve our confidence in delivering adequate dose to the target while minimizing toxicity to nearby OARs. Newer radiotherapy techniques and technologies are also expected to increasingly aid in the reirradiation setting, such as deformable registration, adaptive radiotherapy via Ethos Therapy and MRI-guided adaptive radiotherapy via Elekta Unity, proton therapy, and rectal spacer implantation. Our sample size limits this case report, and future research should study this patient population on a larger scale to provide more precise guidelines for clinicians to navigate these types of cases.
Reirradiation for de novo anorectal cancers in patients with a history of prostate radiotherapy is feasible from a dosimetric perspective. However, approaching these cases require careful consideration of the potential for increased toxicity. Effective collaboration between radiation oncologists and the medical physics team can help mitigate these risks, making it a viable therapeutic option for this unique patient population.
The authors have no conflict of interests to declare.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”
