AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2692-9759/164
President of all nations, Morning star hospital, Enayam Thoppu Kanyakumari District, India
*Corresponding Author: Ramachandran Muthiah, President of all nations, Morning star hospital, Enayam Thoppu Kanyakumari District, India.
Citation: Ramachandran Muthiah, (2025), Giant Vegetation’ of Mitral Valve, Cardiology Research and Reports, 7(4); DOI:10.31579/2692-9759/164
Copyright: © 2025, Ramachandran Muthiah. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 May 2025 | Accepted: 30 May 2025 | Published: 06 June 2025
Keywords: rheumatic mitral valvulitis; infective endocarditis; giant vegetation; flail leaflet; mitral regurgitation; ping-pong mitral stenosis
Infective endocarditis (IE) is the infection of inner endothelial layer of the heart including the heart valves and it may present as rapidly progressive or manifest itself as subacute or chronic disease. The epidemiology of infective endocarditis has been changed over the past few decades and the incidence of IE in children in United States and Canada is 1 in 1,250 pediatric hospital admissions in the early 1980s. Atleast 70% of infective endocarditis in children occurs with congenital heart disease whereas rheumatic heart disease in southern states of India and the degenerative mitral valve disease (myxomatous, mitral valve prolapse) in the western countries are the most underlying predisposing conditions to infective endocarditis in adolescents. The characteristic lesion of infective endocarditis is ‘vegetation’ and a‘large’ vegetation > 10 mm in size has been reported with an incidence 15.9-62.5% of patients. The significance of vegetation size has been a subject of discussion for many years to predict the embolic episodes. Background of this case study illustrated the varying size and shape of giant vegetation attached to the anterior leaflet of mitral valve in an underlying rheumatic mitral valvulitis and its consequence of valve damage such as chordal rupture, flail leaflet and mitral regurgitation with a description of anatomic features and echocardiographic manifestations in a 10-year old female child.
The mitral valve apparatus consists of leaflets, subvalvular apparatus (chordae tendineae and papillary muscle), annulus and the left ventricle. It is a dynamic three-dimensional system that allows brisk left ventricular blood-inflow during diastole and ensures unidirectional heart pump function by sealing the left atrium from left ventricle during systole. The anterior (aortic or septal) leaflet of the mitral valve originates from the fused superior and inferior cushion tissues in the left AV (atrioventricular) canal and starts delaminate or separate from the myocardial wall shortly thereafter. The posterior (mural) leaflet forms from the left lateral cushion. The mitral valve leaflets, chordae and papillary muscles become developed at the 15th week of gestation [1]. The anterior leaflet of the mitral valve is semicircular(trapezoid or dome-shaped) and it is larger, longer and thicker than the posterior leaflet and comprises one third of the annulus circumference and is in fibrous continuity with the left and non-coronary cusps of the aortic valve with the interleaflet triangle between the aortic cusps that abuts on to the membranous portion of the interventricular septum [2]. The posterior (mural leaflet) is quadrangular in shape and comprises two-thirds of the annular circumference. The posterior leaflet has two well defined indentations (clefts) that generally form three scallops (segments) along the elongated free edge. These leaflets are attached at their bases to the fibromuscular ring and by their free edges to the subvalvular apparatus. The commissures define a distinct area where the anterior and posterior leaflets come together at their insertion into the annulus. The leaflets are having a basal zone (connecting to the atrioventricular junction), thin central clear zone and a thick rough zone at the free edge of the leaflets. The rough zone is the main area of chordal attachment, the region of coaptation ( the line of contact between the leaflets) and apposition (overlap of the leaflet free edge). The mitral valve leaflet is tri-laminar, consists of fibrosa/ventricularis, spongiosa and atrialis layers and endothelial cells cover the blood- interfering surfaces. The fibrosa is composed of dense collagen (type I-74%, Type III-24%, type V-2%) [3] and it is providing the strength and stiffness to the leaflets. It is the major load bearing layer that faces the greatest pressure during valve closure, extends from the annulus into two-thirds of the leaflets and it is absent at the free edge. The spongiosa is the major component of the free edge and consists of extracellular matrix or ground substance of glycosaminoglycans and proteoglycans which are hydrophilic and attract water molecules [4]. This characteristic of water absorbent proteins causes the ground substance to expand and swell at the free edge and act as a protective buffer to ensure a tight seal along the point of apposition. Smooth muscle cells, veins and arterioles are confined to the base of the leaflets at the fibrous-myocardial junction where the leaflets inserts. Atrial myocardial cells extend into the base of the leaflets and has dense innervations and excitability, suggest a neural regulatory mechanism [5]. The leaflets have chords (chordae tendineae), the fibrous strings that originate with highly variable branching from papillary muscle tips (heads) and insert fan-like into the ventricular aspects of the leaflets. According to the site of insertion, they are termed as primary or marginal, secondary or intermediate and tertiary or basal chords. Primary chords are inserted on the free edge of the rough zone of both leaflets and function to prevent prolapse or eversion (flail) of the leaflet margin. Secondary chords attach to the ventricular surface on the region of rough zone (ie, body of the leaflet) and relieve tension on the valves. There is a pair of large, thick secondary chords arising from the tip of each papillary muscle to anterior leaflet, termed as ‘strut’ chords, which are thought to be strongest and preserving ventricular shape and function. Tertiary chords are found in posterior leaflet only and attach directly to the ventricular wall [6]. Unlike the tricuspid valve, the mitral valve does not have chords anchoring the leaflets to the ventricular septum.
Complete closure (coaptation) and correct apposition (symmetrical overlap, usually a minimum of 4-5 mm) of both leaflets is essential in preventing regurgitation. Leaflet coaptation depends on the balance of systolic tethering and closing forces on the valve. Tethering forces are transmitted through the LV (left ventricular) wall-papillary muscle-chordal system and keep the leaflets from protruding into the left atrium. Closing forces depend on the pressure generated by the left ventricle to close the mitral valve. Disturbances of this finely tuned spatial and temporal interplay may create an imbalance of these forces and result the valve to become regurgitant. Rheumatic valvulitis may cause mitral regurgitation by retraction of tendinous chords and leaflets as well as annular dilatation, thus compromising coaptation between the two leaflets, leading to regurgitation. Infective endocarditis can cause mitral regurgitation through chordal rupture or leaflet perforation.
Review of literature
Rheumatic disease is the etiology for stenotic mitral valves in > 99% of cases. The cause of pure mitral regurgitation are multiple and include floppy mitral valves, infective endocarditis, papillary muscle dysfunction, rheumatic disease, and ruptured chordae tendineae. In a study by Allen and associates [7], the three leading causes of pure mitral regurgitation were floppy (28%), rheumatic (29%), and idiopathic chordal rupture (14%). In a study by Hanson and colleagues [8], the three leading causes were floppy (70%), papillary muscle dysfunction (24%), and infective endocarditis (2%). In a study by Olson and associates [9], the reported leading causes to be floppy (38%), rheumatic (31%), and papillary muscle dysfunction (11%), but Wallen and colleagues [10] found rheumatic disease accounted for only 3% of purely regurgitant mitral valves.
Endocarditis was first described by William Osler in 1885. It is an inflammatory process that affects the endocardium and may have an infective or noninfective origin. It is uncommon in the western world (22 cases per million), but more prevalent in developing countries and a giant vegetation blocking the mitral valve orifice is uncommon and so this case had been reported.
A 10 year female child was referred for echocardiographic evaluation with an apical systolic murmur. The child was having recurrent episodes of rheumatic fever ( febrile illness with joint pains) at the age of 5-6 years and taken some treatment from the local medical practitioner, but she was not taken penicillin prophylaxis earlier. The child was remained afebrile for long period and no precipitating factors of infective endocarditis such as dental or genitourinary procedures in the past. General examination revealed normal growth and development, no cyanosis and clubbing and peripheral signs of infective endocarditis such s Osler’s nodes, Janeway lesions, Roths spots and splinter haemorrhages are not present and they are relatively rare in children. Physical examination revealed a grade 3/6 , blowing, high pitched, holosystolic murmur with a constant intensity and duration on dynamic auscultation and loudest at the apex with a radiation to left axilla and transmitted to the left infrascapular area and vertebral coloumn and it is due to the flow generating the murmur is directed posterolaterally within the left atrial cavity, suggesting the murmur of mitral regurgitation due to the rupture of chordae tendineae of anterior mitral leaflet. Blood culture revealed normal. Blood chemistry revealed the positive serum ASO titer, suggesting a recent streptococcal infection and other parameters are normal. X- ray chest reveled moderate cardiomegaly and ECG revealed a left ventricular volume overload pattern of eccentric hypertrophy due to LV dilatation as a result of severe mitral regurgitation and a normal rhythm. Transthoracic echocardiography revealed a giant vegetation ‘popcorn’ like in Figures 1,3 and 4 and ‘cucumber’ like in Figure 2, mainly attached to base and apical portion of anterior mitral leaflet as shown in Figure 31 and manifested in various size and shapes as shown in Figures 1 to 33. A flail anterior leaflet with a disorganized mitral regurgitation jet as shown in Figure 16 and 21 and the posterior leaflet is embedded with vegetation and resulting in ‘kissing forms’ as shown in Figures 13, 14 and 15 in echocardiography imaging. Tricuspid valve is also thickened and calcified as shown in Figure 2 in addition to thickened and calcified mitral leaflets, suggesting an underlying rheumatic etiology predisposing to the formation of vegetation. The child was given 1.2 million units of intramuscular benzathine penicillin injection as a therapeutic and initial prophylaxis dose for rheumatic fever and advised every 3 weeks for life long. Small doses of digoxin and diuretics are also prescribed and advised early surgery (mitral valve replacement)
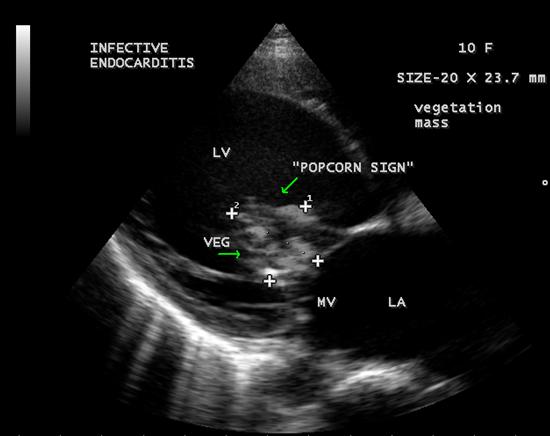
Figure 1: A large ‘popcorn’ like vegetation obstructing the mitral valve-‘ giant vegetation’ [36-Figure 3].
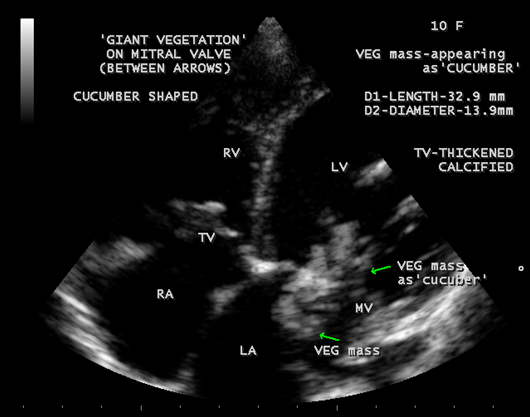
Figure 2: A large ‘cucumber’ like vegetation obstructing the mitral valve- ‘giant vegetation’. TV (tricuspid valve also thickened and calcified due to rheumatic process
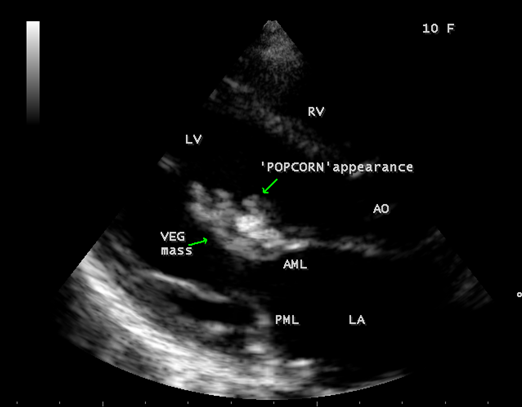
Figure 3: A ‘ Popcorn’ like vegetation attached with anterior mitral leaflet moving into the left ventricle along with valve leaflet
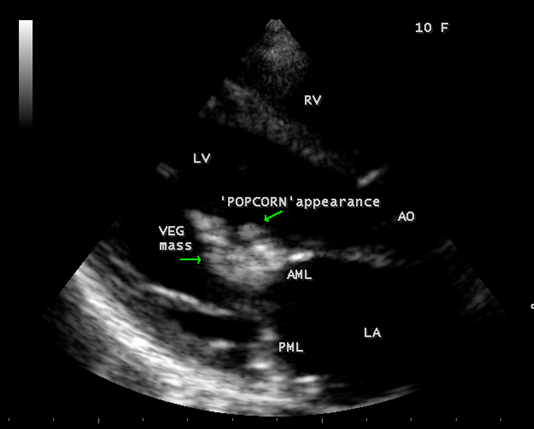
Figure 4: A ‘popcorn’ like vegetation attached with anterior mitral leaflet moving closer to the mitral valve orifice
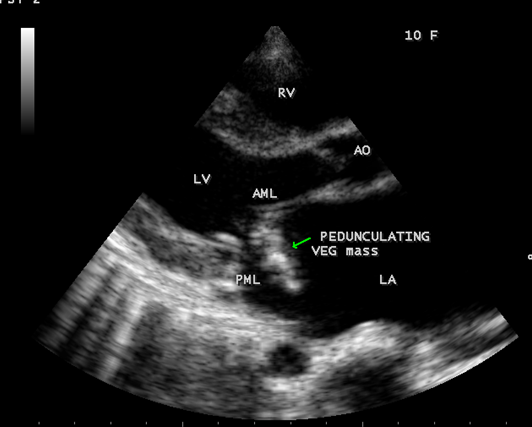
Figure 5: Flail anterior mitral leaflet with a pedunculated, partially calcified, vegetation mass into the left atrium (LA) [33-Figure 13.1]
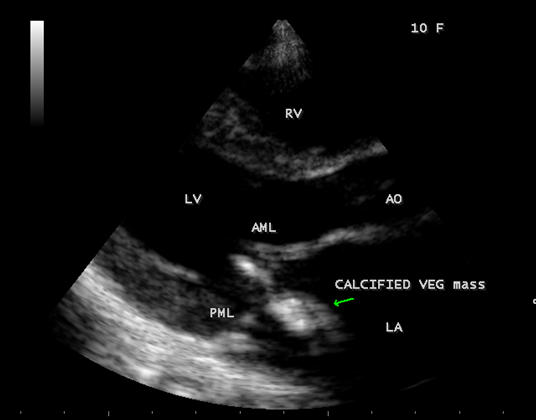
Figure 6: Healed mass of vegetation (calcified) attached with AML (anterior mitral leaflet) into LA (left atrium)
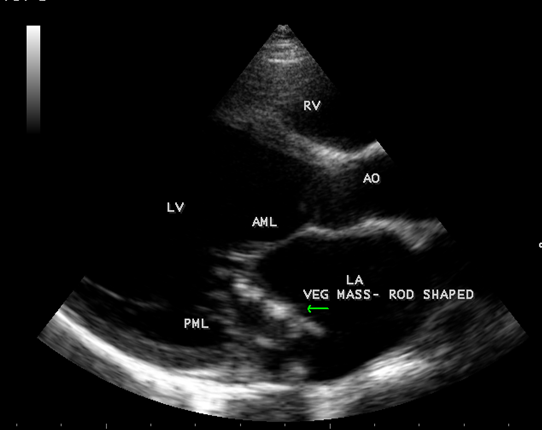
Figure 7: Vegetation seen as ‘ rod-shaped’ into LA (left atrium).

Figure 8: Vegetation seen as attached to the base of AML(anterior mitral leaflet)
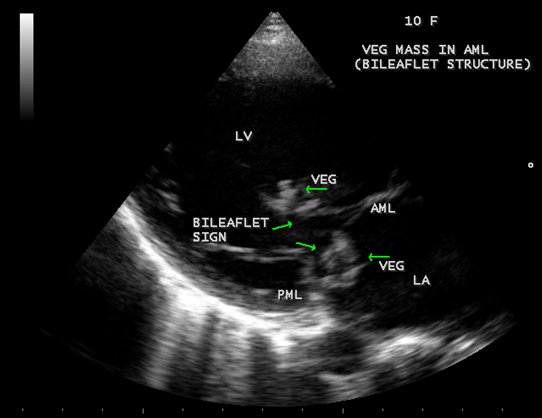
Figure 9: Vegetation seen as ‘bileaflet structure’ attached to AML.
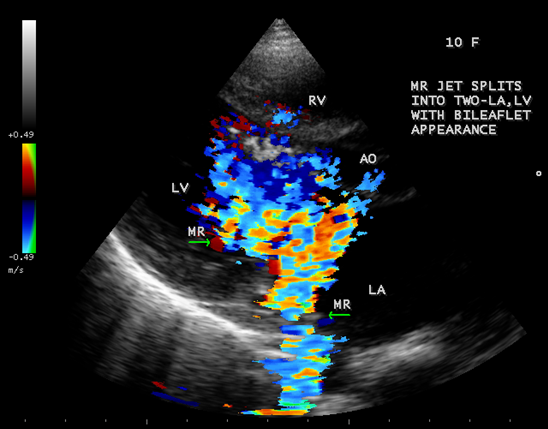
Figure 10: Color Doppler imaging showing the MR (mitral regurgitation) jet as bileaflet appearance- simultaneously into LA and LV.
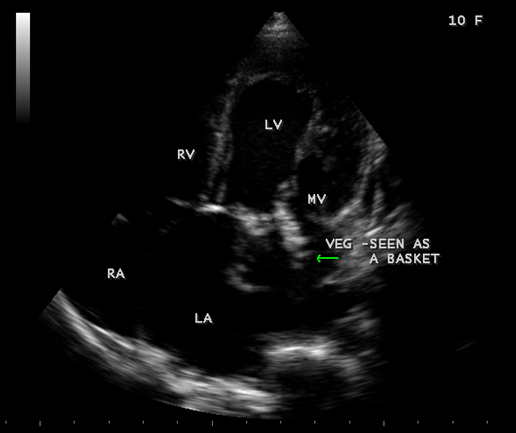
Figure 11: Vegetation seen as ‘basket’ shaped in mitral valve orifice [33-Figure 13.3B]
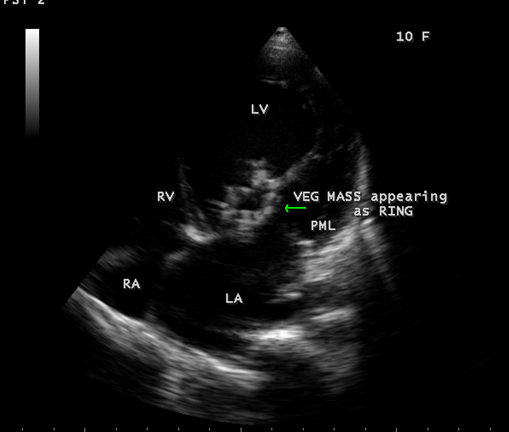
Figure 12: Vegetation seen as ‘ring’ attached to AML.
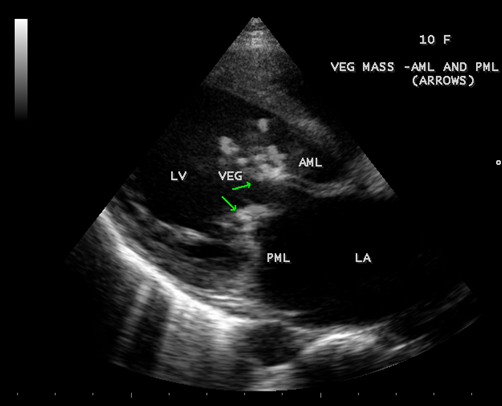
Figure 13: Vegetation seen as ‘kissing’ type in Parasternal long axis view-both AML and PML having the vegetation.
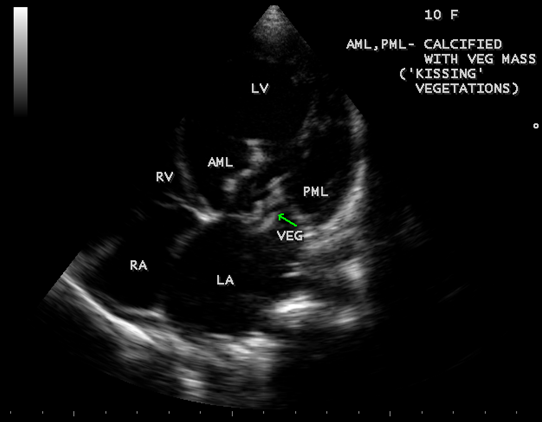
Figure 14: Vegetation seen as ‘kissing’ type in Apical four chamber view.
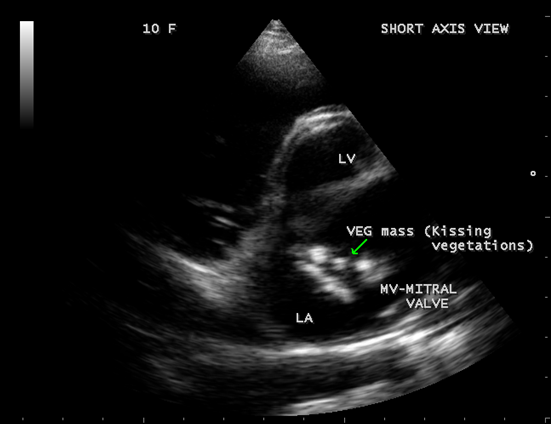
Figure 15: Vegetation seen as ‘kissing’ type in short axis view.
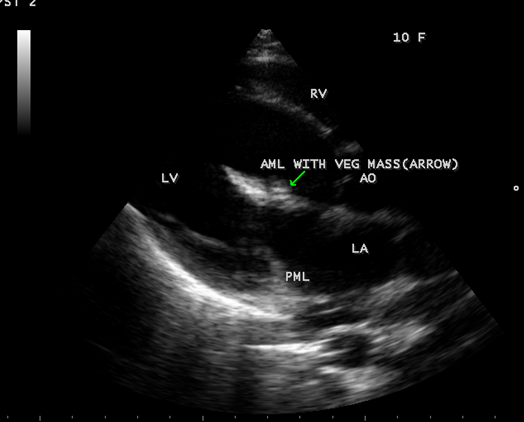
Figure 16: Vegetation embedded on AML in Parasternal long axis view [33-Figure 13.7]
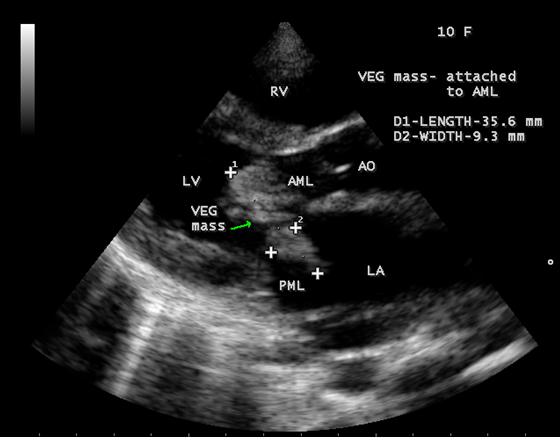
Figure 17: Vegetation attached to AML (anterior mitral leaflet) showing the size in Parasternal long axis view)
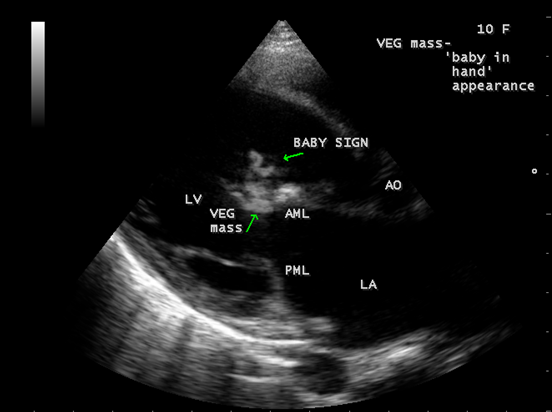
Figure 18: Vegetation seen as ‘baby in hand’ appearance on AML (anterior mitral leaflet)
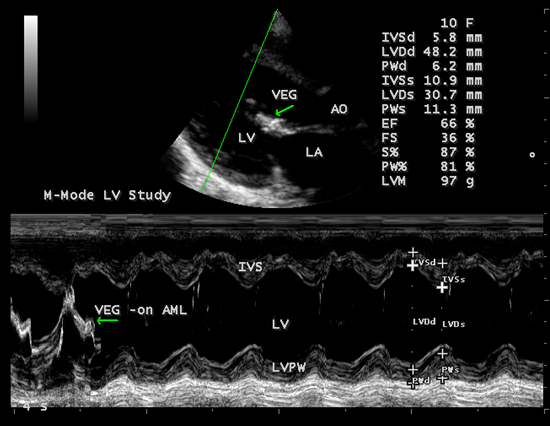
Figure 19: M-mode LV function study
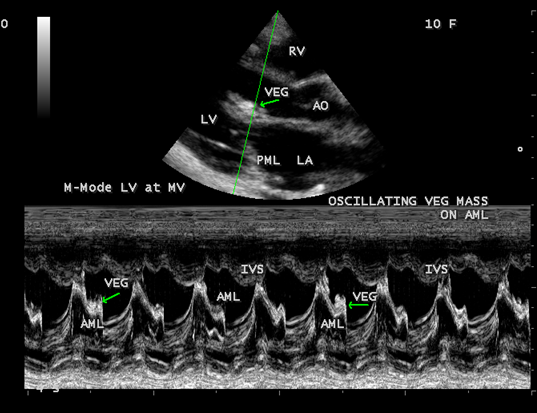
Figure 20: M-mode LV at mitral valve level- showing vegetation on AML
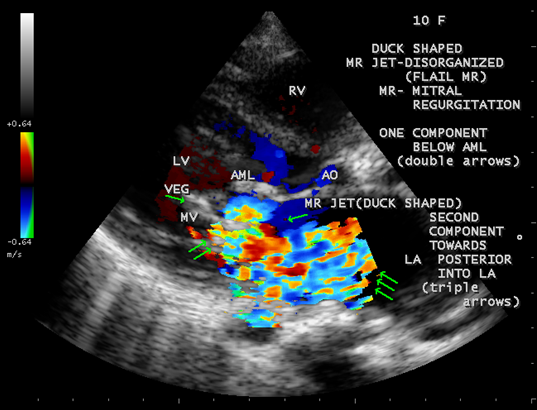
Figure 21: Disorganized MR jet (one component behind AML- double arrows and the second component posterior towards LA-triple arrows))of flail anterior mitral leaflet [33-Figure 11.79]
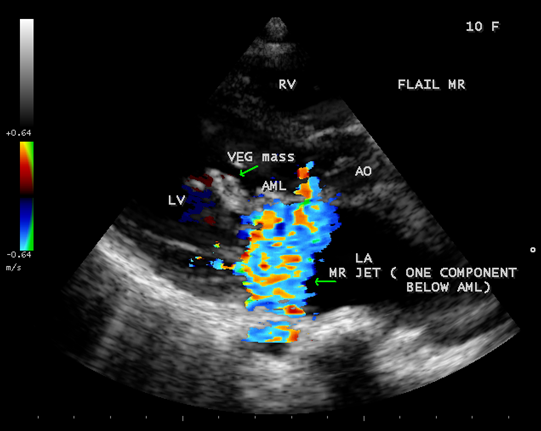
Figure 22: Disorganized Flail MR jet- one component behind AML(anterior mitral leaflet)-Highly eccentric jet..
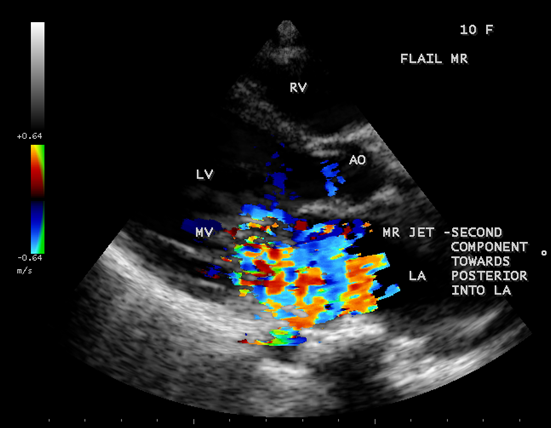
Figure 23: DisorganIzed MR jet – second component posterior towards LA
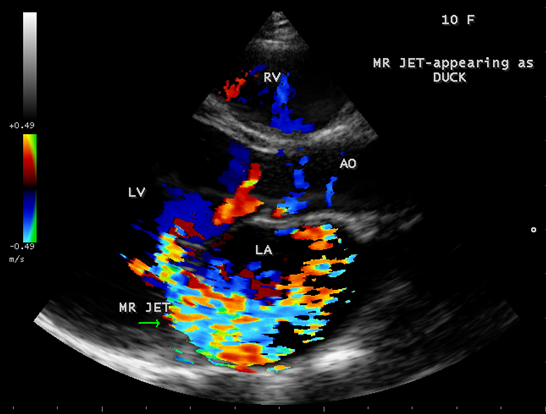
Figure 24: The ‘duck’ shaped MR jet – posterior towards LA
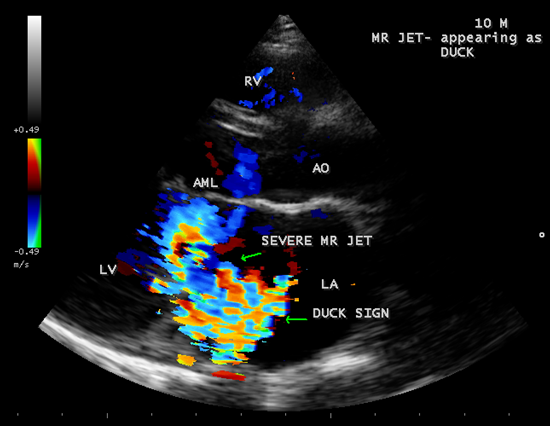
Figure 25: The ‘duck’ shaped MR jet- hugging the LA wall suggesting severe regurgitation
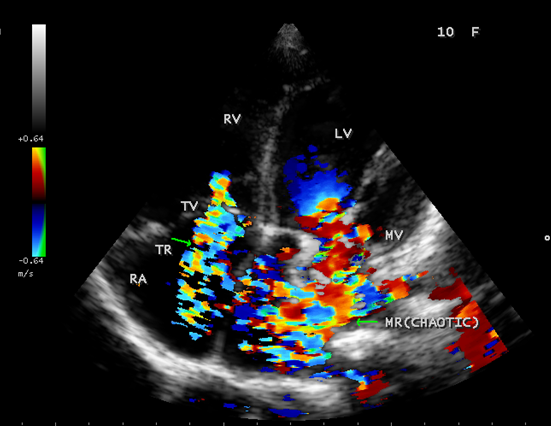
Figure 26: Apical four chamber view showing the chaotic MR (mitral regurgitation) jet, TR ( tricuspid regurgitation) jet.
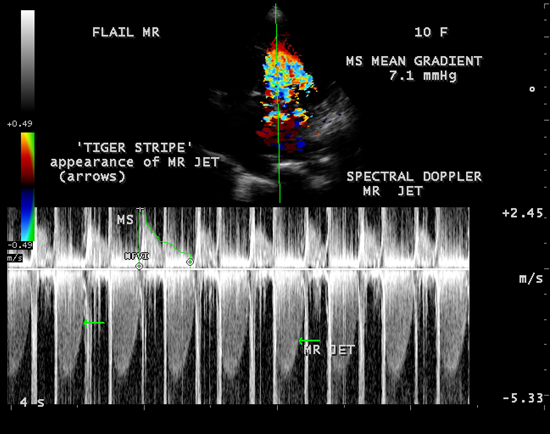
Figure 27: CW Doppler showing the ‘tiger stripe’ appearance (arrows)on spectral Doppler of MR jet due oscillating flail segments in the regurgitant stream[33-Figure 11.85]
The mitral valve apparatus is a very complex structure and all of its components must work together for proper valve function. Mital regurgitation can occur when any one of these elements fails through different mechanisms that affect leaflet coaptation. Intrinsic valvular involvements by degenerative, rheumatic and infective endocarditis produce organic (primary or structural) mitral regurgitation whereas abnormal function of normal leaflets due to impaired ventricular function caused by ischemic heart disease and dilated cardiomyopathy [11], produce functional (secondary)mitral regurgitation as a result of an imbalance between tethering forces ( annular dilatation, LV (left ventricular) dilatation, papillary muscle displacement, LV sphericity) and closing forces (reduced LV contractility, global LV and papillary muscle dyssynchronies and altered mitral systolic annular contraction). Papillary muscle rupture secondary to myocardial infarction defined an organic ischemic MR (mitral regurgitation). A descriptive classification of mechanism was developed by Carpentier in 1983 based upon the movement of leaflets as normal, excessive or restricted [12] as shown in Table-1 by understanding the papillary muscle-chordal-leaflet scaliop relationship which has been defined anatomically by Lam et al and it is modified by Carpentier himself in 1995 to include a mechanism of leaflet restriction during systole causing regurgitation as Type IIIb.
| Types | Leaflet motion | Mechanism |
Type 1
| Normal motion
| Annular dilation, clefts, leaflet perforation |
Type II
|
Excessive motion
|
Prolapse, flail chords, ruptured papillary muscle
|
Type III Type IIIa
| Restricted motion Restriction during diastole and systole
|
Commissural fusion due to rheumatic heart disease
|
Type IIIb
| Restriction during systole only | Chordal tethering, papillary musle displacement
|
Table 1: Mechanism of MR (mitral regurgitation) based on leaflet motion-Carpentier’s functional classification)
Kumar, et al [13] proposed a classification (Duran classification) based on chordal insertion from the two groups of papillary muscles as lateral half of both leaflets is designated with 1 and the medial half with 2.Thus, anterior leaflet is divided into A1 with chordal crossing from the anterolateral papillary muscle and A2 with chordal crossing from the posteromedial papillary muscle. The posterior leaflet scallops are designated as P1(anterolateral) and P2(posteromedial) and a large middle scallop as PM. The PM is a larger scallop and subdivided as PM1 and PM2 based on chordal origin.
When a part of the mitral valve body protrudes into the left atrium beyond the mitral annulus and producing mild regurgitation with a preservation of coaptation is termed as “ billowing valve”. It is stated that the mitral valve billows slightly into the left atrium normally and an exaggerated finding should be termed as “ billowing mitral valve”, extreme form of billowing is “floppy valve” and when chordal rupture, the prolapsed mitral valve is “ flail”. A morphologic abnormality with thickened leaflet ( diastolic thickness > 5 mm) due to redundant tissue is termed “ floppy valve”. When the coaptation line is beyond the annular plane, it is termed as mitral valve prolapse, the leaflet tip is directed towards LV and its most common phenotype is diffuse myxomatous degeneration (Barlow’s disease) in which the middle spongiosa component of the leaflet is unusually prominent and the quantity of acid mucopolysaccharide is increased. When the free edge of the leaflet is completely reversed into the left atrium (LA), the leaflet tip directed towards LA, it is termed as “flail leaflet”, usually as a consequence of chordal rupture[13].. In moderate prolapse, when the leaflet tip remains in the left ventricle, it is called as ‘billowing valve’ and in severe prolapse when the leaflet tips bulges into the left atrium, it is called as ‘flail leaflet”.
Rheumatic valvulitis is characterized by variable thickening of the leaflets at their free edge, chordal fibrosis, rigidity and reduced motion of posterior leaflet in diastole and in some patients, the posterior leaflet remains in a semi-open position throughout the cardiac cycle and the friction of anterior leaflet in systole produce a false aspect of prolapse. This friction causes endothelial damage and results in platelet-fibrin deposition which is more susceptible to colonization by microorganisms. The initially sterile platelet-fibrin nidus called as non bacterial thrombotic endocarditis (NBTE) become secondarily infected by microorganisms circulating in the blood, either from distant source of focal infection as result of transient bacteremia from a mucosal or skin source [14] and establishing an infectious nidus or vegetation on the endocardium and most commonly they are found at the valve closure-contact ( coaptation) line on the atrial surface of the mitral valve [15]. Following successful medical therapy, the vegetative lesions may heal by a process of endothelialization of the surface phagocytes of bacterial debris, sometimes with calcification and subsequent organization by fibroblasts. Vegetation can be attached to any part of the valve and move with the leaflet but in a more chaotic (oscillating) manner and prolapsed through the valve when it opens. Vegetation can prevents leaflet coaptation, and valvular retraction during the healing phase of endocarditis and result in mitral regurgitation. Large vegetation particularly at the mitral valve may result in functional valve stenosis and hemodynamic deterioration [15]. When the infection extends beyond the valve leaflet, distortion of leaflet and chordal rupture may occur, leading to severe regurgitation [16]. Ruptured mitral chordae tendineae (RMCT) are increasingly reported as an important cause of mitral regurgitation [17]. Anterior chordae tendineae rupture of the mitral valve was common in chronic rheumatic valvulitis (CRV) and infective endocarditis. In myxomatous degeneration, the posterior leaflet chordal rupture is more common and the posterior leaflet become ‘flail’ with a ‘saloon door effect’.
Rheumatic mitral regurgitation has a benign course as stated by Bland and James [18] in the analysis of the cases of rheumatic valvular lesions over a 20-year period. Levine and Friedberg have suggested that there are two groups of patients with mitral regurgitation, one group showing rapidly progressive and the other group showing a prolonged, stable and benign course. In most patients with severe primary MR (mitral regurgitation), left ventricular compensation is maintained for years, but ultimately the prolonged hemodynamic overload leads to myocardial decompensation.
Echocardiographic Features
Infective endocarditis is the microbial infection of the endocardial(endothelial) surface of the heart and the formation of vegetation ( a variably sized amorphous mass of platelets and fibrin in which abundant microorganisms and scant inflammatory cells are enmeshed) is the hallmark of the disease and the vast majority of vegetations, however, occur on valve leaflets. The classic approach to the diagnosis of endocarditis by von Reyn does not include echocardiographic findings and it is mainly focused on pathological, clinical and laboratory evidence (positive blood cultures). In 1994, the Duke criteria for the diagnosis of infective endocarditis [20] defined ‘positive echocardiogram’ as vegetation , an oscillating intracardiac mass, a new valvular regurgitation and microbiological evidence was established with a high sensitivity and specificity ( generally about 80%). Steckelberg and Wilson[21] suggest that the incidence of endocarditis in the general population is approximately 5 cases per 100,000 persons-years. Valve redundancy and thickened leaflets (>5mm) by echocardiography identify a population at increased risk for infective endocarditis. The relative risk of infective endocarditis among mitral valve prolapse ranges from 3.5 to 8.2. Rheumatic heart disease is the predisposing cardiac lesion in 20 to 25% of cases in 1970’s and 1980’s[22], in Europe, it is 7-18%[23]. In children, it is less than one in ten cases of infective endocarditis [24] and the mitral valve is most frequently affected in women while the aortic valve in men.
Echocardiography is the only noninvasive method available for direct visualization of endocarditis-induced lesions. Echocardiographic finding in patients with infective endocarditis was initially observed by Dillon [25] and Spangler, et al [26]. The vegetation will grow in size, either as a sessile clump or a highly mobile and even pedunculated mass with the potential for embolization. Vegetation can be detected when the valve attached mass reach a diameter of ≥ 2 to 3 mm [27]. In both children and adults, 2-D echocardiography is usually the more sensitive technique with sensitivity in children up to 80% [28]. Valvular dysfunction due to tissue disruption or large obstructing vegetation can be visualized and quantitated by echocardiogram with Doppler [29]. The detection of a large eccentric jet adhering, swirling, and reaching the posterior wall of the LA is in favour of significant MR (mitral regurgitation) as shown in Figures 22, 24 and 25.
Vegetation
The most common and direct evidence of infective endocarditis is the vegetation and it begins as a microscopic focus of infection and gradually grows into a conspicuous mass. It is typically an irregularly shaped, highly mobile, echogenic mass attached to the free edge of a valve leaflet ( most commonly at the coaptation line) and tends to develop on the ‘upstream’ side of the valve leaflets ( ie, the ventricular side of aortic valve and the atrial side of mitral and tricuspid valves. They may be seesile or pedunculated, but usually has an oscillating or fluttering motion, a typical feature of most vegetations. Vegetation move with the leaflet in a more chaotic (‘oscillating’) manner and it may prolapse through the valve into the LV (left ventricle) as it opens as shown in Figures 3, 4 and 16 and into LA (left atrium) as it closing (Figure 5 and 6) . The mass of vegetation is typically homogeneous with echogenicity similar to that of the myocardium. The infectious process often alter the valvular structure and function. Extensive involvement of the leaflet may result in chordal rupture, leading to severe regurgitation as shown in Figure 21 . Direct and typical signs of RMCT (ruptured mitral chordate tendineae) were chain-flail or whiplash-like changes and had an incidence of 86.7%, causing severe regurgitation and mitral chordal rupture is the leading cause of flail mitral leaflet[30]. A large vegetation may obstruct the valve orifice as shown in Figure 1 and 2 , sometimes termed as “obstructive-type bacterial endocarditis” and producing a functional valve stenosis ( Ping-Pong mitral stenosis [31]) similar to left atrial myxoma as shown in Figure 29.
The shape and size of vegetation are quite variable and mostly it is polypoid [32]. The typical vegetation is a ‘sessile’ or ‘ pedunculating’ valve – attached mass. A ‘sessile’ vegetation had to be completely attached to the valve as shown in Figures 34 and 35 in a 63- year old male, in which a large vegetation is attached to the atrial side of anterior mitral leaflet [33-Figure 13.3-A], producing severe mitral regurgitation as shown in Figure 36 and a mobile vegetation showed a pedunculating part prolapsing into the ventricle as shown in Figure 3 and 4 or atrium as shown in Figure 5 [33-Figure 13.1] in a 10-year old female child. A vegetation was considered as ‘definite’ when shaggy echoes in the M-mode study as shown in Figure 20 . and a corresponding mass without restricted valve motion in the two-dimensional echocardiogram were found as shown in Figure 16 and 30 [33-Figure 13.7]. The vegetation vary in size, often being just a few mm and sometimes reaching to 2-3 cm. A vegetation must be atleast 3 to 6 mm in size to be reliably seen. The mean size of vegetation was 0.6 mm (range 3 to 28) and vegetation > 10 mm in diameter was defined as ‘large’ and those ≤ 10 mm in diameter was defined as ‘small’ and ≥ 15 mm is ‘very large’. Vegetations resulting from fungal infections (candida, aspergillus) are usually much bigger than bacterial vegetations and can be so big to be mistaken for a cardiac tumor. The large vegetations are at increased risk for embolic complications [34], especially on the anterior leaflet of the mitral valve with mobility [35]. A vegetation size of 3.2 x 4.4 cm is called as ‘giant vegetation’ on the mitral valve with a fibrillary appearance of the mass [36- Figure 3] as shown in Figure 1 is an important predictor of embolic phenomena in patients with infective endocarditis causing severe mitral regurgitation as ‘Duck’ shaped jets (Figures 24 and 25 ), disorganized (Figure 21) and sometimes the regurigitant jet splits into two components as one into LA and the second one into LV simultaneously as a bileaflet jets (Figure 10 ) similar to bileaflet structure of AML with vegetation masses (Figure 9 ) . The size of the largest vegetation reported on the mitral valve in the literature in patients with bacterial endocarditis is 7x4 cm[37]. In a study of Nunes, et al[38], vegetation size >13 mm was the only independent predictor of mortality, but some studies [39],[40] did not had an increased embolic risk in patients with vegetation focused only on its presence and size and not on their location. Embolic complications may occur in infective endocarditis(20.6%)and were not more prevalent in the groups with large vegetations [41]. However, Wong, et al [42] found an increased need for surgery in patients with a large vegetation (>10 mm).
The size and shape of vegetation vary due to curling of vegetation. The size of vegetation in this child is 35.6 x 9.3 mm as in Figure 17 , 20 x 23.7 mm as in Figure 1, 32.9 x 13.9 mm as in Figure 2 .
The shape of vegetation varies in this child as ‘popcorn’ like (Figures 1,3 and 4 ), rod-shaped (Figure ), basket shaped (Figure 7 )[33-Figure 13.3], ‘baby in hand’ appearance (Figure 18), ‘cucumber shaped (Figure 2 ) and a ‘bunch of plantain’appearance (Figure 33 ), ring shaped (Figure 19 }, bileaflet structure (Figure 9 )with bileaflet MR jet as shown in Figure 10 . and kissing forms (Figure 13 - parasternal long axis view, Figure 14 - apical four chamber view and Figure 15 - short axis view)
‘Flail’ Mitral Regurgitation (MR)
The anatomic disruption of a portion of the mitral valve apparatus dueto the underlying rheumatic valvulitis with predisposing infective endocarditis which form a vegetation , resulting an eccentric regurgitation jet with orientation opposite in direction of the leaflet having the anatomic defect such as ‘flail’. In the presence of ‘flail leaflet’, the mitral regurgitant spectral signal may have an atypical appearance and the flail portion oscillate in the spectral signal of regurgitant flow stream to produce a ‘tiger stripe’ appearance as shown in Figure 27. associated with ‘whistling’ sound on auscultation[33-Figure 11.85]. The mitral regurgitation (flail MR) jet is chaotic as shown in Figure 26, highly eccentric (Figure 22) and disorganized with one component behind the anterior mitral leaflet and the second component directed towards posterior immediately as in Figure 21 [33- Figure 11.79].
The severity of eccentric MR is underestimated because of coanda effect. If the regurgitant jet area fills < 20% of the left atrium, it is mild and > 40% indicate severe regurgitation. The vena contracta ( the neck or narrowest portion of the jet), typically imaged perpendicular to the commissural line in parasternal long axis and apical four chamber views is well defined in both central and eccentric jets, but not in chaotic, disorganized jets due to flail leaflets. Its width < 3 mm indicates mild MR , > 7 mm defines severe MR and a mean value of > 8mm indicates severe functional MR. The flow convergence method based on PISA (proximal isovelocity surface area) may not applicant for eccentric and multiple jets or complex and elliptical regurgitant orifices to assess the severity of mitral regurgitation.. The adaptation of LV to the increased volume overload is reflected by LV dimensions and ejection fraction. In chronic compensated phase, the forward stoke volume is maintained through an increase in LV ejection fraction >65% and the patient could be asymptomatic. In chronic decompensated phase of MR, the forward stroke volume decreases and the LA pressure increase significantly. The patient may be still asymptomatic and the LV ejection fraction may be in the low normal range despite the presence of significant muscle dysfunction. The contractile function decreases silently and become irreversible. In the current guidelines, surgery is recommended in asymptomatic patients with severe organic MR when the LV ejection fraction is ≤ 60%. However, in acute stage, the LV ejection fraction increases in response to the increased preload. The end-systolic diameter is less preload dependent than the ejection fraction and it may be more appropriate to monitor the global LV function. The end-systolic diameter > 45 mm also indicate the need for mitral valve surgery [43]. In this child, the LVESD (end-systolic diameter) is 30.7 mm and the ejection fraction (EF) is 66% as shown in Figure 19. New parameters are currently available for a better assessment of LV function. A systolic tissue Doppler velocity measured at the lateral annulus<10.5 cm/s has been shown to identify significant LV dysfunction and to predict post-operative LV function in patients with asymptomatic organic MR [44]. Strain imaging allows a more accurate estimate of myocardial contractility than tissue Doppler velocities. In MR, strain has been shown to decrease even before LV end-systolic diameter exceeds 45mm[45]. A resting longitudinal strain rate <1.07/s(average 12 basal and mid segments) is associated with subclinical latent LV dysfunction [46]and a global longitudinal strain <18.1% has been associated with post operative LV dysfunction[47]. The left atrium dilates in response to chronic volume and pressure overloads. LA remodelling (diameter >40-50mm) may predict the onset of atrial fibrillation and poor prognosis in patients with organic MR[48]. The excess regurgitant blood entering in the LA may induce acutely or chronically a progressive rise in pulmonary pressure and the presence of TR (tricuspid regurgitation) as shown in Figures 26 and 28 permits the estimate of systolic pulmonary arterial pressure and mitral valve surgery is recommended when it is > 50 mmHg at rest and LA reverse remodeling may occur after surgery. The severe TR may cause a decrease in hepatic vein systolic velocity and systolic flow reversal may occur as shown in Figure 32 and its sensitivity is 80% [49]. The TR (tricuspid regurgitation) jet velocity in this child is 4.03 m/s as shown in Figure 28 which corresponds to a systolic pulmonary artery pressure of 65 mmHg.
Treatment
Pharmacological Therapy
Pharmacological therapy aims to alleviate symptoms and to prevent the progression of LV dysfunction. Afterload reduction is of particular benefit in the management of both acute and chronic forms of mitral regurgitation [50]. Afterload reduction with sodium nitroprusside is life saving in acute conditions such as chordal or papillary muscle rupture. It stabilizes the patient by reducing the impedence to the LV ejection and thus, the regurgitant volume and LA pressure decrease. Dobutamine may be administered along with nitroprusside if hypotension exists. Afterload reduction in chronic, severe MR with vasodilators such as angiotensin converting enzyme inhibitors are beneficial in presence of heart failure, but not beneficial in its absence [51]. In addition to diuretics, digitalis glycosides are indicated in patients having severe MR and heart failure, particularly with established atrial fibrillation in addition to anticoagulants, IE prophylaxis was advised during surgical procedures in these patients.
Surgical Therapy
Asymptomatic patients with severe MR having excellent ventricular function (EF > 70%, ESD(end-systolic diameter) < 40 mm) can be safely followed by a ‘ watchful waiting approach” until symptoms, LV dysfunction (EF ≤ 60%, ESD ≥ 45 mm) and pulmonary hypertension develops. Mitra valve surgery is the only treatment for MR which provides substantial relief of symptoms and prevent the development of heart failure [52]. The normal function of the mitral valve apparatus ‘ primes” the left ventricle for normal contraction.. Operative procedures may interfere the annular-chordal-papillary muscle continuity, may results in postoperative LV dysfunction and so the preservation of these structure are now considered as a critical feature of MVR ( mitral valve replacement)[53]. Reconstructive procedures are carried out in degenerative MR due to mitral valve prolapse and chordal rupture as well as in ischemic functional MR[54]. Percutaneous cather-based mitral valve repair procedures such as leaflet edge-to-edge repair and mitral annular reduction are currently under clinical evaluation and the preliminary results are encouraging [55]. The severely deformed valves in rheumatic heart disease are not suitable for reconstructive surgery and they require MVR[56] and the operation should be desirable before they develop marked LV dysfunction [57] and serious symptoms since severe LV dysfunction(EF < 30%) may cause high perioperative mortality[58]. Excellent survival is observed in patients with ESD < 45 mm , EF ≥ 60% and the 5-year survival rate is 40% in ischemic MR and 75% in rheumatic MR.. Intermediate outcome may occur when LV ESD is 45-52 mm and the ejection fraction between 50-60%. Poor outcome is associated with values below these limits.
Surgery may be considered in mobile vegetation >10 mm in size since the incidence of systemic embolization are increased (33%) compared to those with smaller size (19%) and particularly those on anterior mitral leaflet are uniquely associated with embolic episodes. Urgent surgery is indicated when a large vegetation is associated with embolic events, heart failure and persistent infection[59]. In patients with valvular dysfunction and in whom the infection is controlled with antibiotic therapy and cardiac function is compensated, surgery may be delayed until antimicrobial therapy has been completed. Early surgery is appropriate in patients with large vegetation who may need valve replacement in future since larger vegetations are associated with increased risk of mortality and embolization[60],[61]. Some authors suggest that the causative microorganism is associated with embolic complications rather than the size of vegetation [62]
Since this child is having a giant vegetation with disorganized severe mitral regurgitation due to flail anterior mitral leaflet as the result of chordal rupture, the child was advised MVR(mitral valve replacement) with mechanical prostheses along with removal of vegetation and to continue penicillin prophylaxis with anticoagulant therapy for life long. Since the vegetation is healed, partially calcified, organized mass, the antimicrobial regimen for infective endocarditis was not administered. The anticoagulant therapy is not preferred at this moment since the child had no embolic episodes and the role of prophylactic anticoagulant therapy is questionable in presence large vegetation in the absence of atrial fibrillation, The child was advised small doses of digoxin and diuretics along with penicillin prophylaxis.
Several factors play a role in the prognosis of IE(infective endocarditis). Costa,et al described the clinical and echocardiographic scores as the predictors of mortality in infective endocarditis. Age > 40 years ( 4 points), class IV heart failure ( cardiogenic shock)(4 points), uncontrolled sepsis (6 points), conduction disease(5 points), arrhythmias(8 points), a valve with excessive damage (5 points), large and mobile vegetation(4 points)[63]. Mortality rates for scores below 10 were 5.26% and the scores over 20 were 78.9%. The child is having a large and mobile vegetation (4 points), extensive valve damage (5 points) and according to this study, the mortality rate of this child is 5.26%.
A giant vegetation attached to the anterior mitral leaflet and presented with various shapes in a 10-year old female child was described by Transthoracic 2D echocardiography imaging. The child had underlying rheumatic involvement of the mitral valve and the infective endocarditis causing chordal rupture leading to flail anterior mitral leaflet with severe mitral regurgitation. The vegetation functionally obstructing the mitral orifice and results in’ Ping- Pong’ mitral stenosis due to mass effect. The child remained asymptomatic without any embolic episodes and heart failure symptoms on follow up of two years.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

I would like to express my sincere gratitude for the support and efficiency provided by the editorial office throughout the publication process of my article, “Delayed Vulvar Metastases from Rectal Carcinoma: A Case Report.” I greatly appreciate the assistance and guidance I received from your team, which made the entire process smooth and efficient. The peer review process was thorough and constructive, contributing to the overall quality of the final article. I am very grateful for the high level of professionalism and commitment shown by the editorial staff, and I look forward to maintaining a long-term collaboration with the International Journal of Clinical Case Reports and Reviews.

To Dear Erin Aust, I would like to express my heartfelt appreciation for the opportunity to have my work published in this esteemed journal. The entire publication process was smooth and well-organized, and I am extremely satisfied with the final result. The Editorial Team demonstrated the utmost professionalism, providing prompt and insightful feedback throughout the review process. Their clear communication and constructive suggestions were invaluable in enhancing my manuscript, and their meticulous attention to detail and dedication to quality are truly commendable. Additionally, the support from the Editorial Office was exceptional. From the initial submission to the final publication, I was guided through every step of the process with great care and professionalism. The team's responsiveness and assistance made the entire experience both easy and stress-free. I am also deeply impressed by the quality and reputation of the journal. It is an honor to have my research featured in such a respected publication, and I am confident that it will make a meaningful contribution to the field.

"I am grateful for the opportunity of contributing to [International Journal of Clinical Case Reports and Reviews] and for the rigorous review process that enhances the quality of research published in your esteemed journal. I sincerely appreciate the time and effort of your team who have dedicatedly helped me in improvising changes and modifying my manuscript. The insightful comments and constructive feedback provided have been invaluable in refining and strengthening my work".

I thank the ‘Journal of Clinical Research and Reports’ for accepting this article for publication. This is a rigorously peer reviewed journal which is on all major global scientific data bases. I note the review process was prompt, thorough and professionally critical. It gave us an insight into a number of important scientific/statistical issues. The review prompted us to review the relevant literature again and look at the limitations of the study. The peer reviewers were open, clear in the instructions and the editorial team was very prompt in their communication. This journal certainly publishes quality research articles. I would recommend the journal for any future publications.

Dear Jessica Magne, with gratitude for the joint work. Fast process of receiving and processing the submitted scientific materials in “Clinical Cardiology and Cardiovascular Interventions”. High level of competence of the editors with clear and correct recommendations and ideas for enriching the article.

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.

My article, titled 'No Way Out of the Smartphone Epidemic Without Considering the Insights of Brain Research,' has been republished in the International Journal of Clinical Case Reports and Reviews. The review process was seamless and professional, with the editors being both friendly and supportive. I am deeply grateful for their efforts.

To Dear Erin Aust – Editorial Coordinator of Journal of General Medicine and Clinical Practice! I declare that I am absolutely satisfied with your work carried out with great competence in following the manuscript during the various stages from its receipt, during the revision process to the final acceptance for publication. Thank Prof. Elvira Farina

Dear Jessica, and the super professional team of the ‘Clinical Cardiology and Cardiovascular Interventions’ I am sincerely grateful to the coordinated work of the journal team for the no problem with the submission of my manuscript: “Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report).” The review process by 5 experts was fast, and the comments were professional, which made it more specific and academic, and the process of publication and presentation of the article was excellent. I recommend that my colleagues publish articles in this journal, and I am interested in further scientific cooperation. Sincerely and best wishes, Dr. Oleg Golyanovskiy.

Dear Ashley Rosa, Editorial Coordinator of the journal - Psychology and Mental Health Care. " The process of obtaining publication of my article in the Psychology and Mental Health Journal was positive in all areas. The peer review process resulted in a number of valuable comments, the editorial process was collaborative and timely, and the quality of this journal has been quickly noticed, resulting in alternative journals contacting me to publish with them." Warm regards, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. I appreciate the journal (JCCI) editorial office support, the entire team leads were always ready to help, not only on technical front but also on thorough process. Also, I should thank dear reviewers’ attention to detail and creative approach to teach me and bring new insights by their comments. Surely, more discussions and introduction of other hemodynamic devices would provide better prevention and management of shock states. Your efforts and dedication in presenting educational materials in this journal are commendable. Best wishes from, Farahnaz Fallahian.

Dear Maria Emerson, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. I am delighted to have published our manuscript, "Acute Colonic Pseudo-Obstruction (ACPO): A rare but serious complication following caesarean section." I want to thank the editorial team, especially Maria Emerson, for their prompt review of the manuscript, quick responses to queries, and overall support. Yours sincerely Dr. Victor Olagundoye.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. Many thanks for publishing this manuscript after I lost confidence the editors were most helpful, more than other journals Best wishes from, Susan Anne Smith, PhD. Australian Breastfeeding Association.

Dear Agrippa Hilda, Editorial Coordinator, Journal of Neuroscience and Neurological Surgery. The entire process including article submission, review, revision, and publication was extremely easy. The journal editor was prompt and helpful, and the reviewers contributed to the quality of the paper. Thank you so much! Eric Nussbaum, MD

Dr Hala Al Shaikh This is to acknowledge that the peer review process for the article ’ A Novel Gnrh1 Gene Mutation in Four Omani Male Siblings, Presentation and Management ’ sent to the International Journal of Clinical Case Reports and Reviews was quick and smooth. The editorial office was prompt with easy communication.

Dear Erin Aust, Editorial Coordinator, Journal of General Medicine and Clinical Practice. We are pleased to share our experience with the “Journal of General Medicine and Clinical Practice”, following the successful publication of our article. The peer review process was thorough and constructive, helping to improve the clarity and quality of the manuscript. We are especially thankful to Ms. Erin Aust, the Editorial Coordinator, for her prompt communication and continuous support throughout the process. Her professionalism ensured a smooth and efficient publication experience. The journal upholds high editorial standards, and we highly recommend it to fellow researchers seeking a credible platform for their work. Best wishes By, Dr. Rakhi Mishra.

Dear Jessica Magne, Editorial Coordinator, Clinical Cardiology and Cardiovascular Interventions, Auctores Publishing LLC. The peer review process of the journal of Clinical Cardiology and Cardiovascular Interventions was excellent and fast, as was the support of the editorial office and the quality of the journal. Kind regards Walter F. Riesen Prof. Dr. Dr. h.c. Walter F. Riesen.

Dear Ashley Rosa, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews, Auctores Publishing LLC. Thank you for publishing our article, Exploring Clozapine's Efficacy in Managing Aggression: A Multiple Single-Case Study in Forensic Psychiatry in the international journal of clinical case reports and reviews. We found the peer review process very professional and efficient. The comments were constructive, and the whole process was efficient. On behalf of the co-authors, I would like to thank you for publishing this article. With regards, Dr. Jelle R. Lettinga.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, I would like to express my deep admiration for the exceptional professionalism demonstrated by your journal. I am thoroughly impressed by the speed of the editorial process, the substantive and insightful reviews, and the meticulous preparation of the manuscript for publication. Additionally, I greatly appreciate the courteous and immediate responses from your editorial office to all my inquiries. Best Regards, Dariusz Ziora

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation, Auctores Publishing LLC, We would like to thank the editorial team for the smooth and high-quality communication leading up to the publication of our article in the Journal of Neurodegeneration and Neurorehabilitation. The reviewers have extensive knowledge in the field, and their relevant questions helped to add value to our publication. Kind regards, Dr. Ravi Shrivastava.

Dear Clarissa Eric, Editorial Coordinator, Journal of Clinical Case Reports and Studies, Auctores Publishing LLC, USA Office: +1-(302)-520-2644. I would like to express my sincere appreciation for the efficient and professional handling of my case report by the ‘Journal of Clinical Case Reports and Studies’. The peer review process was not only fast but also highly constructive—the reviewers’ comments were clear, relevant, and greatly helped me improve the quality and clarity of my manuscript. I also received excellent support from the editorial office throughout the process. Communication was smooth and timely, and I felt well guided at every stage, from submission to publication. The overall quality and rigor of the journal are truly commendable. I am pleased to have published my work with Journal of Clinical Case Reports and Studies, and I look forward to future opportunities for collaboration. Sincerely, Aline Tollet, UCLouvain.

Dear Ms. Mayra Duenas, Editorial Coordinator, International Journal of Clinical Case Reports and Reviews. “The International Journal of Clinical Case Reports and Reviews represented the “ideal house” to share with the research community a first experience with the use of the Simeox device for speech rehabilitation. High scientific reputation and attractive website communication were first determinants for the selection of this Journal, and the following submission process exceeded expectations: fast but highly professional peer review, great support by the editorial office, elegant graphic layout. Exactly what a dynamic research team - also composed by allied professionals - needs!" From, Chiara Beccaluva, PT - Italy.

Dear Maria Emerson, Editorial Coordinator, we have deeply appreciated the professionalism demonstrated by the International Journal of Clinical Case Reports and Reviews. The reviewers have extensive knowledge of our field and have been very efficient and fast in supporting the process. I am really looking forward to further collaboration. Thanks. Best regards, Dr. Claudio Ligresti

Dear Chrystine Mejia, Editorial Coordinator, Journal of Neurodegeneration and Neurorehabilitation. “The peer review process was efficient and constructive, and the editorial office provided excellent communication and support throughout. The journal ensures scientific rigor and high editorial standards, while also offering a smooth and timely publication process. We sincerely appreciate the work of the editorial team in facilitating the dissemination of innovative approaches such as the Bonori Method.” Best regards, Dr. Matteo Bonori.
