AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2641-0419/418
President of all Nations Morning star hospital, Enayam Thoppu, Kanyakumari District, Tamil Nadu state, India.
*Corresponding Author: Ramachandran Muthiah President of all Nations Morning star hospital, Enayam Thoppu, Kanyakumari District, Tamil Nadu state, India.
Citation: Ait Yahya AE, Ztati Simohammed, Noussaiba Malhabi, Imane Katif, Mohammed EL Jamili, et al, (2024), “End-stage” Constrictive Pericarditis- Stem cell Therapy, J Clinical Cardiology and Cardiovascular Interventions, 7(12); DOI: 10.31579/2641-0419/418
Copyright: © 2024, Noussaiba Malhabi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 September 2024 | Accepted: 30 October 2024 | Published: 29 October 2024
Keywords: ‘end-stage’ constrictive pericarditis; engorged neck vein; septal bounce; waffle procedure; amniotic stem cell therapy
Aim: To present a case of ‘end-stage’ constrictive pericarditis with clinical manifestations such as ascites mimicking as cirrhosis of liver.
Introduction: ‘End-stage’ constrictive pericarditis has been readily confused with cirrhosis of liver in which there may be ascites, but venous pressure is normal and the neck veins are not engorged. There may be cardiac enlargement in other causes of heart failure. Etiology remains unknown in majority of case and inflammatory process play a central role in its development.
Case Report: A 67-year old male presented with sudden onset of tachycardia. Clinical examination revealed right-sided heart failure, ‘Egg-shell’ calcification in Chest X-ray and a characteristic echocardiographicfeatures of pericardial constriction such as septal bounce and dynamic respiratory changes in mitral inflow velocity. The patient was advised medical measures since it is in advanced stage.
Conclusion: When clinical signs of right heart failure become unresponsive to increased doses of diuretics, constrictive pericarditis is more likely the underlying disease since severe, right-sided failure develops in very advanced, the end-stage of the disease.
The normal pericardium is a fibroelastic sac surrounding the heart and consists of two layers. The visceral pericardium (serous pericardium) is a single layer of mesothelial cells contiguous with epicardium and reflects on itself over the origin of great vessels up to 1 to 2 cm and pulmonary veins. A tough, fibrous layer as a parietal pericardium and the sac created by these layers contain a small amount of fluid (< 25>
A 67-year old male was admitted with sudden onset of palpitations in the emergency room. ECG revealed tachycardia with a heart rate of 150 bpm as in Figure 4 and blood pressure 110/70 mmHg. Blood chemistry revealed normal. Physical examination showed an engorged neck vein as shown in Figure 2 which fails to decrease with inspiration (Kussmaul’s sign) with a deep Y descent (Freidreich’s sign) reflecting the predominant ventricular filling during early diastole, ascites and pedal edema as shown in Figure 1 suggesting a right-sided heart failure. Auscultation revealed pericardial knock, an early diastolic sound occurs due to cessation in diastolic filling and retraction of apical impulse in systole. X-ray chest revealed “egg-shell’ calcification as shown in Figure 3. Transthoracic echocardiography revealed the features of constrictive pericarditis as in Figures 7 to 12. Since the patient is in end-stage disease, he was given conservative medical measures such as diuretics, antibiotics and anti-inflammatory drugs and the rhythm was controlled with calcium channel antagonist, verapamil 40 mg three times daily as shown in Figures 5 and 6.

Figure 1: Showing the clinical features of ‘end-stage’ Constrictive pericarditis.

Figure 2: Showing the ‘engorged neck vein’ as a feature of elevated venous pressure in ‘end-stage’ constrictive pericarditis
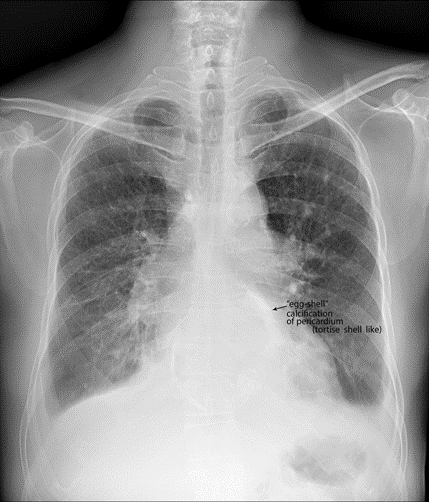
Figure 3: X-ray chest PA (postero-anterior) view showing the ‘egg-shell’ calcification’ – ‘tortoise-shell’ like and flattening of right heart border in ‘end-stage’ constrictive pericarditis.
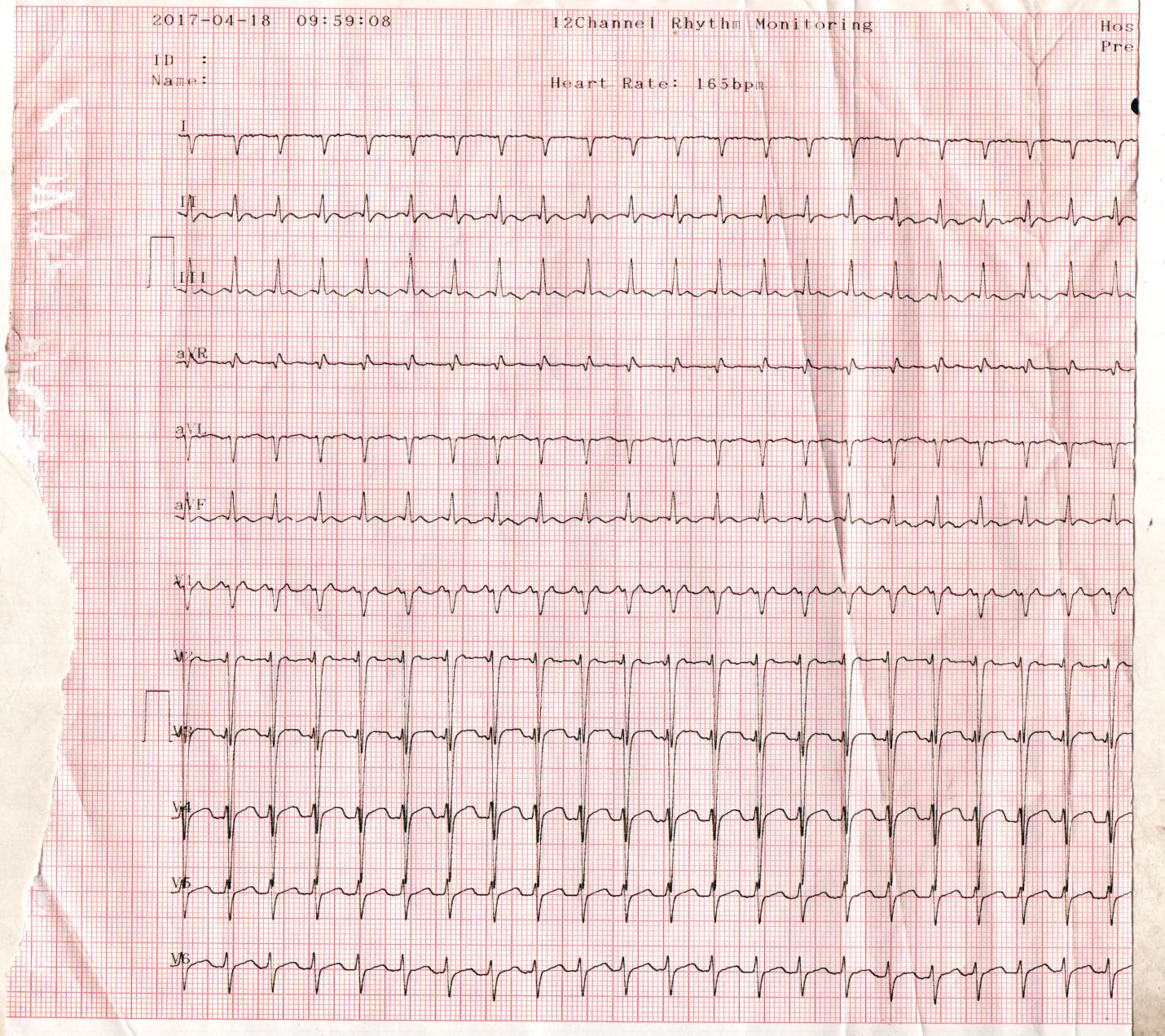
Figure 4: ECG showing tachycardia (rate 150 bpm) in a 67 year old male with ‘end-stage’ constrictive pericarditis.
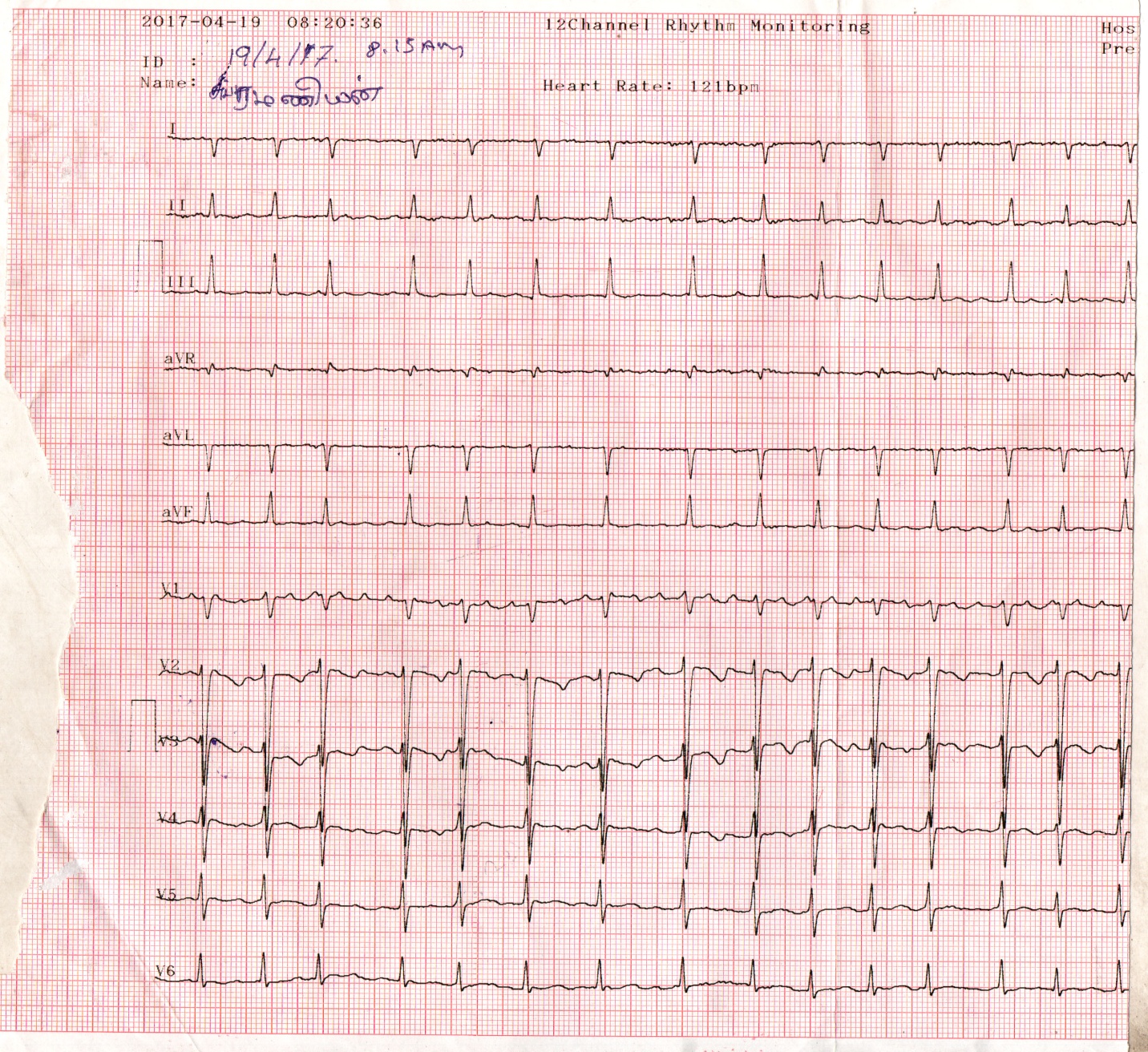
Figure 5. ECG showing atrial fibrillation after controlling the heart rate with verapamil

Figure 6: ECG normalizing on continuation of verapamil

Figure 7: Showing the ‘ acute angle’ between the LA (left atrium) and LV(left ventricle) posterior walls and a pericardial thickness of 8 mm.

Figure 8: Apical view showing the ‘septal bounce’ as a sign of ventricular interdependence and bulging of IAS (interatrial septum) towards LA (left atrium).

Figure 9: M-mode LV study showing the ‘septal notch’ and ‘ dip and flattening’ of LV posterior wall

Figure 10: Pulsed Doppler imaging showing ‘the dynamic respiratory change’ of the mitral inflow velocity of constrictive pattern.


Figure 11: Pulsed Doppler imaging showing the expiratory increase in diastolic IVC flow reversal in both phases of respiration, but more prominent in expiration

Figure 12: Subcostal view showing the dilated IVC (inferior vena cava- plethoric ) with no respiratory variation.

Figure 13: Pulsed Doppler imaging showing the mitral inflow velocity with no respiratory variation of restrictive pattern.

Figure 14: Showing the IVS (interventricular septum) calcification in effusive-constrictive pericarditis as evidenced by mild pericardial effusion with an associated disease of Endomyocardial fibrosis.
Review of literature
In 1669, Lower [2] described the clinical effects of interference of cardiac diastole by a constricting fibrous pericardium. In 1756, Morgagni [3] contributed to the understanding of pathophysiology of constrictive pericarditis. In 1828, Lancisi described the characteristic syndrome of constrictive pericarditis and in 1842 [4], Chevers was the first to present clearly the clinical picture of chronic constrictive pericarditis. In 1870, Wilks [5] further emphasized this syndrome. In 1896, Pick [6] described the postmortem evidence of adhesive pericarditis and an atypical fibrosis (pseudocirrhosis) of the liver and its capsule in patients with constrictive pericarditis. The thickened peritoneum over the liver is not to be the engorgement of liver itself in so-called Pick’s disease, but rather to the occurrence of acute peritonitis at the time of acute pericarditis followed by residual fibrosis. Concato described the effusion in serous cavities (polyserositis) in patients with constrictive pericarditis is due to the result of cardiac compression, and inflammation of serous membranes is absent or occur secondarily.
Etiopathogenesis
Constrictive pericarditis is most commonly caused by conditions or events that cause inflammation to develop around the heart. Inflammatory process of the pericardium typically causes pain and fluid accumulation and more chronically results in fibrosis and calcification of pericardium with pericardial constriction, the process that inhibit diastolic filling of the heart. The most common antecedents are idiopathic and tuberculosis. In many cases, the etiology is not identified, however, pericardial fibrosis and calcification are often idiopathic in origin [7]. The tuberculosis accounted for 49% of cases of constrictive pericarditis in a series reported in 1962 [8] and it was found to be most common cause in third-world countries such as India [9],[10]. Viral pericarditis is more common in the west and in Europe and North, it is often a sequelae of cardiac surgery and mediastinal irradiation.
Constrictive pericarditis can occur after many pericardial disease process. All causes of pericarditis can lead to subsequent constriction [11]. Rheumatic fever, although frequently accompanied by pancarditis, does not result in chronic constrictive pericarditis and may have pericardial adhesion which are not maximally constricting. The pericarditis associated with uremia and with myocardial infarction is not of the constricting type and most cases of effusive-constrictive pericarditis are often idiopathic, can occur in malignancy of breast and lung, tuberculosis and hypothyroidism (cholesterol pericarditis or ‘gold paint’ pericarditis) The causes of constrictive pericarditis are shown in Table 1
| Most common | Less common |
Idiopathic -42 to 49 % [12] Mediastinal irradiation (5-10 years duration) Following Cardiac surgery-11 to 37 % (post-pericardiectomy-10 to 40 %, previous cardiac surgery-0.3 %) Radiotherapy- 9 to 31 % Post-infectious- 3 to 6 % Tuberculosis-49 % (the most common cause In developing countries) Viral infections (coxsackie virus A and B, Adenovirus, echovirus Pyogenic infections
| Other infections Neoplasms -5-17 % (lung-33 %, breast-25 %, adenocarcinoma of intestine [13]) Connective tissue disorders (rheumatoid Arthritis, systemic lupus erythematosis, Scleroderma) Drugs(procainamide,hydralazine,methysergide) Trauma Hereditary-Mulibrey nanism(Mu-muscle, Li-liver, br-brain, ey-eyes, nanism-dwarf) in Finland and United states [14] |
Table 1: showing the causes of constrictive pericarditis
Hemodynamic changes
The normal pericardium can stretch to accomodate the physiological changes in cardiac volume. In constrictive pericarditis, the visceral and parietal pericardium are fibrosed and fused together [15], although not necessarily always thickened [16], prevent the heart from expansion and resulting in minimal ability to adapt to volume changes and significant dynamic respiratory variation in blood flow in the chambers of the heart attributed to isolation of the cardiac chambers from intrathoracic respiratory pressure changes, ie, dissociation between intrathoracic and intracardiac pressures with enhanced ventricular interaction as reported by Hatle et al in 1989 [17].
In the heart with a normal pericardium, inspiration causes a decrease in intrathoracic pressure, which is reflected in the cardiac chambers as decrease in intracardiac pressures simultaneously and there is no change in the driving pressure from the lungs across the pulmonary veins into the left atrium and across the mitral valve into the left ventricle. There is some increase in the filling of the right ventricle because of enhanced venous return, but filling of the left ventricle is unaffected throughout the cardiac cycle. In patients with constrictive pericarditis, the rigid pericardium does not allow the decrease in intrathoracic pressure to be transmitted to the left -sided chambers and there is a lower driving force from the lungs into the left side of the heart and the left ventricle becomes underfilled with a reciprocal increase in the filling of the right ventricle and therefore a septal shift occurs [18]. Conversely, during expiration, there is decreased filling of the right ventricle and increased filling of the left ventricle. As both ventricles are sharing the same limited space, the chamber size and function of one ventricle affect the other ventricle and this interaction is known as ‘ventricular interdependence’ since the amount of blood flow into one ventricle is dependent on the amount of blood flow into the other ventricle and it is enhanced in constrictive pericarditis with a discordance in right and left heart fillings.
Once the ventricular diastolic filling reaches the limitations of the pericardial restraint, the pressure and volume in the cavity rise, filling ceases, and congestion occurs [19]. If the right heart chambers are predominantly constricted, there is naturally an engorgement of neck veins as shown in Figure 2, which is constantly engorged in 86% of patients with constrictive pericarditis. The decreased compliance of right ventricle causes a rise in right atrial pressure that is greater than the fall in pleural pressure, ultimately leading to distended neck veins during inspiration [20], called as ‘Kussmaul’s sign’, which may be seen in right ventricular failure, right ventricular infarction, tricuspid stenosis and restrictive cardiomyopathy. It is nonspecific for constrictive pericarditis and reflects an elevation of Jugular venous pressure (JVP) on inspiration rather than the expected decrease in JVP. When the right heart fails because of constriction of left heart chambers, it may simulate the effect of tricuspid valve disease. With more severe constriction, the peripheral edema and ascites occur. In constrictive pericarditis, the ascites occurs early, disproportionately prominent as well as recurrent and appropriately called as ‘ascites praecox’, followed by minimal edema as a manifestation of later part (end-stage) of the disease and it is usually confined to lower extremities and sacrum whereas in congestive heart failure, the edema appears first and ascites much later.
In isolated constrictive pericarditis, the myocardium is unaffected and therefore the systolic function and early diastolic filling are normal. In the mixed form (constrictive-restrictive- mainly due to radiation –induced, post cardiac surgery), atrophy of myocardial cells and fibrosis may develop during long-term compression by the pericardium. Both the irritation of the heart by the actual process involving the myocardium and the constricting effect of left heart chambers on the right ventricle and right atrium result in atrial arrhythmias such as atrial fibrillation as shown in Figure 5 and less commonly atrial flutter as complications in chronic constrictive pericarditis. With diminution in the output of heart, the blood pressure, especially the pulse pressure tends to be low and the blood pressure decreasing even to the point of disappearance during inspiration, manifested as absence of pulse, an important sign called as ‘paradoxical pulse’ in some of the more advanced cases. Pulsus paradoxus is an exaggeration of normal decrease in systolic blood pressure during inspiration and is formally defined as an inspiratory decrease in systolic blood pressure greater than 10 mmHg during quiet breathing (readily detected by sphygmomanometer, when the reduction is >20 mmHg- it can be detected by simple palpation of brachial artery, severe cases-inspiratory disappearance of pulse) and it is commonly associated with cardiac tamponade, but can be seen occasionally in other conditions such as effusive-constrictive pericarditis, acute severe asthma, acute pulmonary embolism and right ventricular infarction. Normally, the systolic pressure varies with respiratory cycle, but not to the extent seen in pulsus paradoxus. During inspiration, the right ventricle distends due to increased venous return and causes the interventricular septum to bulge into the left ventricle, decreasing the capacity for left ventricular filling and causing a pooling of blood into the pulmonary vessels, which in turn results in a decrease in left ventricular stroke volume, manifested as an exaggerated decrease in the systolic blood pressure [21]. ‘Reversed pulsus paradoxus’(an inspiratory rise in arterial pressure) may occur in hypertrophic obstructive cardiomyopathy [22] and aortic regurgitation tends to prevent the development of pulsus paradoxus despite the presence of cardiac tamponade and it may be absent when the LV and RV diastolic pressure is high or decompression of respiratory changes in pressures as in atrial septal defects. The venous pressure, on the other hand, is very much elevated and frequently exceeding 200 mm of H2O, even exceeding 300 mm of H2O. The salient features of end-stage constrictive pericarditis are shown in Table 2.
High venous pressure Diminution of blood pressure Paradoxical pulse Atrial fibrillation Ascites Low cardiac output (cardiac index = ≤ 1.2 L/m2/minute) Pseudocirrhosis Pedal edema |
Table 2. showing the salient features of constrictive pericarditis
Diagnostic Methods
Radiological The plain radiograph is frequently abnormal in patients with hemodynamically significant constrictive pericarditis [23]. A typical X-ray chest of a patient with constrictive pericarditis shows a normal sized heart (47%) or only mildly enlarged (16%) and moderate to marked enlargement (37%) in effusive-constrictive pericarditis [24]. Cardiac contour abnormalities, particularly the flattening of right cardiac border is a characteristic feature of constrictive pericarditis, but infrequently present. The left atrium, which is covered only partly by the pericardium may be enlarged.
Calcification of pericardium on chest X-ray strongly suggests constrictive pericarditis in patients with features of heart failure ( especially right heart failure) and it is more obvious in regions where the normal fat is found, namely in atrioventricular and interventricular grooves. A localized form of constriction in the mid ventricular segments as a result of localized severe calcification resembling a ‘napkin’ ring shape is termed as “ napkin-ring” constrictive pericarditis [25]. Once calcification has developed, it represents chronic pericarditis and it was present in 40
“End-stage” constrictive pericarditis has posed a diagnostic dilemma since it presented with features of right-sided heart failure such as dyspnea, ascites, edema and elevated JVP (Jugular venous pressure) [95]. Approximately 9% of patients with acute pericarditis go on to develop constrictive physiology. The most important diagnostic tool is clinical suspicion and cardiac catheterization is no longer performed to diagnose it [96]. Two-dimensional echocardiography is used mainly to rule out other causes of right-sided heart failure and Doppler echocardiography may provide additional diagnostic information and confirm the presence of constrictive physiology. Medical therapy may be used as a palliative measure to control symptoms and to optimize hemodynamics in ‘end-stage’ disease, who are not candidates for surgery [97].
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
